

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor,
There are three types of BCR-ABL1 fusion transcripts that differ on the basis of the breakpoint in the BCR gene [1]. The major type, encoding p210, has two isoforms, b2a2 (e13a2) and b3a2 (e14a2), and is associated with more than 95% of Ph-positive CML cases. The minor type, encoding p190, is e1a2. The micro type, encoding p230, is e19a2. This micro type is rare, and has been associated with a variety of hematologic malignancies including neutrophilic CML (CML-N), all phases of classical CML, essential thrombocythemia (ET), and acute myeloid or lymphoblastic leukemia [23]. Here, we describe the first case of chronic phase CML concurrently expressing e1a2 and e19a2 BCR-ABL1.
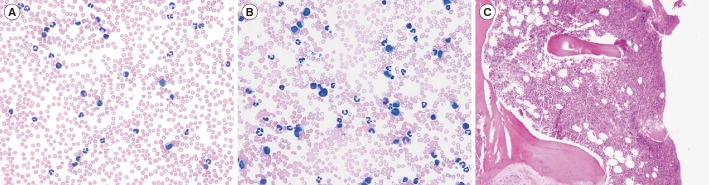
An 89-year-old woman was referred to our hospital for evaluation of her leukocytosis. She appeared ill, but had no splenomegaly. The complete blood count (CBC) revealed 137.46×109/L WBC, 10.0 g/dL Hb, and 194×109/L platelets. The blood smear demonstrated 3% blasts, basophilia, and eosinophilia, and bone marrow (BM) aspirate showed a hypercellularity (Fig. 1). The karyotype in BM was 46,XX,t(9;22)(q34;q11.2) [20] and the FISH result using an LSI BCR/ABL probe (Abbott Molecular Inc., Des Plaines, IL, USA) was nuc ish (ABLx3),(BCRx3),(ABL con BCRx2)[200/200]. JAK2 mutation was not detected.
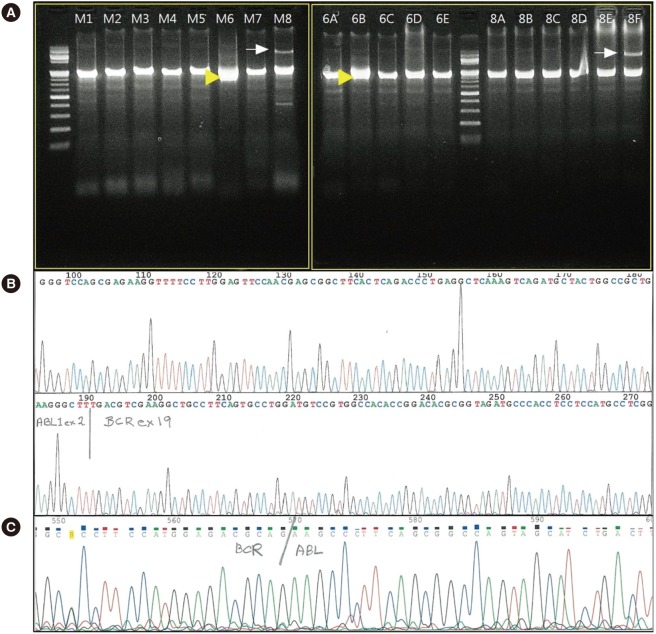
The commercial multiplex reverse transcription (RT)-PCR (HemaVision, DNA Diagnostic, Risskov, Denmark) result was positive for BCR/ABL in Master M6 and Split-out M6B PCR, and presented as an atypically thick band overlapping with the control band at 911 bp (Fig. 2A). Additional sequencing from the M6B amplicon revealed the BCR-ABL1 fusion was the micro type (e19a2) (Fig. 2B). Another real-time quantitative PCR for the minor BCR-ABL1 rearrangement indicated positivity (0.04, normalized copy number [NCN]), which was confirmed by sequencing (Fig. 2C). Therefore, it was determined that the patient had a BCR-ABL1 fusion consisting predominantly of the micro isoform (e19a2) with a small amount of the minor isoform (e1a2). The concurrence of those two isoforms might occur as a result of alternative splicing of the primary BCR-ABL1 fusion transcript [4].
The patient could not start any targeted therapy owing to her poor performance status and the potential interaction with her ongoing risperidone treatment. Only hydroxyurea (500 mg/day) was initiated. One month later, her WBC count decreased to 14.23×109/L. After 6 months, she showed no complications and her WBC count was 16.60×109/L.
The e19a2 BCR-ABL1 fusion transcript can be associated with three types of CML phenotypes, including CML-N, which is characterized by moderate and persistent neutrophilia, absent or minimal splenomegaly, and a benign clinical course [2]. Among typical CML, chronic phase CML presents with significant basophilia, marked splenomegaly, and elevation of circulating immature granulocytes [5]. Atypical CML with thrombocytosis (>1,000×109/L) presents as low WBC count, high platelet count, and mild or absent splenomegaly, having a clinical course featuring ET [6]. The present case was a typical CML in the chronic phase, but lacked marked splenomegaly and monocytosis. The hyperleukocytosis (>100×109/L) seen in this case is usually seen in more advanced, accelerated, or blast phases of CML. However, a case presenting in the chronic phase of CML with e19a2 was reported; the patient eventually worsened to blast crisis [7]. So, hyperleukocytosis could be an indicator of poor prognosis in chronic phases of CML carrying the e19a2 BCR-ABL1 transcript.
The e1a2 is present in 1-2% of typical CML in all phases, but especially in the chronic phase. Monocytosis is a typical feature of CML with e1a2, and is associated with a poor response to tyrosine kinase inhibitors [8]. In the present case, no monocytosis was observed, seemingly owing to the minimal expression of e1a2.
Some reports have described the frequency of the concurrence of two BCR-ABL1 isoforms. Small amounts of the p190 transcript have been observed and are attributed to alternative BCR splicing in more than 90% of patients with CML that predominantly express the p210 transcript [9]. So, the concurrence of two isoforms is not uncommon in CML patients. However, there have been no reports on the concurrence of p230 and p190 transcripts in CML patients.
It is necessary to determine the incidence and clinical impact of the concurrence of p230 and p190 BCR-ABL1 isoforms through further evaluation.
 XML Download
XML Download