

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Cervical intraepithelial neoplasia (CIN) diagnoses have increased in Korea due to periodic screening and the development of cervical cancer examination methods including human papillomavirus (HPV) tests. HPV infection is a cause of premalignant and malignant epithelial lesions of the cervix. Approximately 40 different known HPV genotypes infect the anogenital tract, of which at least 12 genotypes have been linked to the development of CIN [1,2].
The etiological link between HPV genotypes and cervical cancer has been established. Lorincz et al. [3] used the terms low-risk, intermediate-risk, and high-risk to categorize HPV types: low-risk (HPV 6, 11, 42, 43, and 44), which are detected in low-grade CIN but are rare in invasive cancers; intermediate-risk (HPV 31, 33, 35, 51, 52, and 58), which are detected more frequently in CIN than in invasive cancers; high risk/HPV 16, which is associated equally with CIN and invasive carcinoma, and high risk/HPV 18 (HPV 18, 45 and 56), which is more prevalent in invasive cancers than in CIN.
CIN lesions do not always progress to invasive lesions. Spontaneous regression rate in biopsy-proven CIN1 cases is about 60% to 85%. Lesions generally regress, typically within 2 years. CIN2 lesions regress in 40% of cases and persist in 40%. CIN3 lesions regress in 33% of cases but progression to frank carcinoma is about 12% to 22% of cases [4,5]. Hence, it is likely that CIN1/CIN2 represents a less advanced stage of cervical neoplasia than CIN3 including carcinoma in situ (CIS). CIN1/CIN2 versus CIN3+ (CIN3 and CIS) may therefore serve as a measure of the severity of cervical neoplasia.
The loop electrosurgical excision procedure (LEEP) is the preferred treatment for CIN and has some advantages over other methods. However, residual/recurrent disease after a conization procedure using this technique varies between 5% and 30%, requiring reassessment and treatment once lesions are identified [6].
The main purpose of observing patients after LEEP due to CIN is the early detection of residual/recurrent cervical disease presenting a risk of progression to invasive carcinoma if an effective treatment is not administered. The status of resection margins is a predictor of residual disease [7]. Current follow-up protocols are mainly based on periodic cytology.
The relative importance of the different HPV genotypes for the development of CIN is not clear, and the effect of specific HPV genotypes on prognosis in CIN patients treated with LEEP is an open question. In this study, we identified the HPV genotypes more common in CIN3+ compared to CIN1/CIN2. In addition, the effect of specific HPV genotypes on the status of resection margin and prognosis in CIN patients was evaluated.
Materials and methods
1. Case selection
From January 2007 to December 2009, 545 women were diagnosed with CIN and treated by LEEP in our hospital. Ninety-nine women were excluded because they did not have HPV testing, leaving 446 women who had undergone HPV testing at the time of diagnosis to be included in this study. The histological analyses were confirmed with colposcopic-guided biopsy or LEEP. The diagnostic criteria followed the WHO classification of cervical neoplasia.
The HPV genotype was categorized as follows; 1) negative, 2) low-risk (HPV 6, 11, 42, 43, and 44), 3) intermediate-risk (HPV 31, 33, 35, 51, 52, and 58), 4) high risk/HPV 16, 5) high risk/HPV 18 (HPV 18, 45, and 56), and 6) unclassified. The severity of CIN was categorized as CIN1/CIN2 versus CIN3+. CIN3+ included CIN3 and CIS. The specific HPV genotype according to severity of CIN was analyzed.
At follow-up exams, conventional cytology or liquid based cytology technique (Thin Prep, Cytyc Corporation, Boxborough, MA, USA) was performed. The 2001 Bethesda System was used for terminology for reporting the results of the cervical cytology. Margin status by HPV genotypes and progression free survival (PFS) were analyzed in 355 women with three months or more of follow-up. We excluded 91 patients who did not revisit our hospital after LEEP or patients with less than three months of observation following surgery.
Patients were tracked for a median duration of 11 months (range, 3-54 months). Progression was defined as abnormal cytology including atypical squamous cells (ASC), low-grade squamous intraepithelial lesion (LSIL), and high-grade squamous intraepithelial lesion (HSIL).
2. Human papillomavirus testing
For HPV genotyping, a commercially available HPV DNA Chip was purchased from Biomedlab Co. (Seoul, Korea). The manufacturer's protocol describes the preparation and testing of specimens, and the genotyping experiment was performed using a procedure provided by Biomedlab Co. The target HPV DNA was amplified by the polymerase chain reaction (PCR) using the primers (HPV and β-globin) and conditions provided by Biomedlab Co. and labeled using Cy5-dUTP (NEN Life Science Products Inc., Boston, MA, USA). The PCR product was hybridized onto the chip at 40℃ for 2 hours and washed with 3× SSPE and with 1× SSPE for 2 minutes each. Hybridized signals were visualized with a DNA Chip Scanner (GSI Lumonics, Scanarray lite, Ottawa, ON, Canada).
3. Statistical analysis
The statistical analyses were performed with PASW ver. 18.0 (SPSS Inc., Chicago, IL, USA). The specific HPV genotype by severity of CIN and margin status by HPV genotypes were analyzed with Pearson's chi-square test or Fisher's exact test. As independent prognostic factors for PFS, the margin status and HPV genotypes were evaluated by the Kaplan-Meier method with the log-rank test, and multivariate Cox proportional hazard analysis with hazard ratio (HR) and 95% confidence interval (CI). Null hypotheses of no difference were rejected if P-values were less than 0.05, or, equivalently, if the 95% CIs of risk point estimates excluded 1.
Results
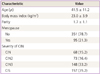
The mean age of all 446 patients was 41.5 ± 11.2 years old, and the mean body mass index was 23.0 ± 3.9 kg/m2. The average parity was 1.7 ± 1.1 and 95 patients (21.3%) were menopausal women. By category of CIN severity, CIS was the most common (157 cases, 35.2%) followed by CIN3 (148 cases, 33.2%), CIN2 (73 cases, 15.2%), and CIN1 (68 cases, 15.2%) in sequence (Table 1).
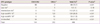
Among the HPV genotypes high risk/HPV 16 was predominant (120 cases, 26.9%), followed by intermediate risk (112 patients, 25.1%), negative (88 cases, 19.7%), unclassified (68 cases, 15.2%), high risk/HPV 18 (53 cases, 11.9%), and low risk (5 cases, 1.1%) in sequence (Table 2). For the analysis of the specific HPV genotype by severity of CIN, each HPV genotype distribution was compared with all other HPV genotypes aggregated. In the negative group, all 88 patients were diagnosed as CIN1/CIN2. In the low risk group, all five patients were diagnosed as CIN3+. In the intermediate risk group, all 112 patients were diagnosed as CIN3+. In the high risk/HPV 16 group, all 120 patients were diagnosed as CIN3+. In the high risk/HPV 18 group, all 53 patients were diagnosed as CIN3+. In the unclassified group, 56 patients were diagnoses as CIN1/CIN2 and 12 patients were diagnosed as CIN3+. Negative (P < 0.01) and unclassified (P < 0.01) group were more common in women with CIN1/CIN2 than CIN3+. Intermediate risk (P < 0.01), high risk/HPV 16 (P < 0.01) and high risk/HPV 18 (P < 0.01) were significantly more common in women with CIN3+ than CIN1/CIN2 (Table 2).
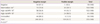
Margin status by HPV genotypes was analyzed in 355 women with 3 months or more of post-treatment information. In the negative group, 54 patients (91.5%) had negative margins and 5 patients (8.5%) were positive. In the intermediate risk group, 73 patients (70.9%) had negative margins and 30 patients (29.1%) positive. In the high risk/HPV 16 group, 58 patients (56.9%) were negative and 44 patients (43.1%) had positive margins. In the high risk/HPV 18 group, 17 patients (41.5%) had negative margins while 24 patients (58.5%) were positive. In the unclassified group, 44 patients (88.0%) had negative margin and 6 patients (12.0%) had positive margin. The proportion of the positive margin was significantly different (P < 0.01) by HPV genotypes and highest in high risk/HPV 18 group (Table 3).
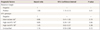
PFS according to the status of margin and HPV genotype was analyzed in these 355 patients. In univariate analysis, only the status of margin had significant effect (P < 0.01) on PFS (Fig. 1). PFS was significantly lower in the positive margin group than the negative margin group (Fig. 1A). The slightly lower PFS observed in the high risk/HPV 18 could be explained by chance (Fig. 1B). By multivariate Cox's proportional hazard analysis, the margin status was the only statistically significant factor affecting PFS (Table 4).
Discussion
HPV 16 and 18 increase the risk of high-grade cervical neoplasia compared to the HPV genotypes aggregated. The association between the specific HPV genotype and prognosis in CIN patients treated with LEEP is not clear, so, we designed this study to evaluate the effect of the specific HPV genotypes on severity and prognosis in CIN patients. Furthermore, we evaluated the effect of specific HPV genotypes on the status of resection margin, a predictor of residual disease in CIN patients treated with LEEP.
Comparisons among studies of HPV genotype and risk of CIN are difficult, since study designs, grouping of HPV genotypes and outcome measures differ among studies. Lorincz et al. [3] recruited 2,627 women into eight studies analyzing the relationship between HPV infection and cervical neoplasia and defined four categories (intermediate risk, high risk/HPV 16, and high risk/HPV 18). Based on these four categories, we classified HPV genotypes into six groups, adding negative and unclassified groups.
We categorized severity of CIN as CIN1/CIN2 versus CIN3+ because CIN1/CIN2 may represent a less advanced stage of cervical neoplasia than CIN3+. Most CIN1 lesions regress spontaneously if untreated. Generally, women diagnosed with CIN2 are treated with excision. However, there is increasing awareness that not all CIN2 is "precancer" [8]. In fact, a large proportion of CIN2 lesions may resolve without treatment, leading to recommendations not to treat CIN2 immediately in young women [9].
In Korea, HPV prevalence is 11.8% among cytologically normal women [10], 73.2% among those with LSIL [11], and 86.4% among those with HSIL [12]. Based on pooled estimates of 11 published papers, the most common high-risk HPV types in HSIL were HPV 16, 52, 58, 51, and 18. The most frequent high-risk HPV types among women with LSIL were HPV 16, 52, 51, 56, and 58. HPV 16 remains the most common HPV type across the range of cervical lesions in Korea [13]. In a cross-sectional study in Norway, including 643 women with CIN2, CIN3 and CIS, HPV 16 was the most common HPV genotype, detected in 51.2% of the women, followed by HPV 31, 33, 52, 18, 51, 58, and 45 [14]. In our study, high risk/HPV 16 was the most common genotype. Intermediate risk, negative, unclassified, high risk/HPV 18 and low risk followed high risk/HPV 16 in order of frequency. We categorized HPV 31, 33, and 52 as intermediate risk.
As for HPV genotypes by severity of CIN, the distribution of HPV types in the CIN1 women and the CIN2/CIN3 women showed a slightly different pattern. In a prospective study in Korea, including 78 CIN patients, the most frequent types in the CIN2/CIN3 women were HPV 16 (29%) and then HPV 58 (13%), 31, 33, and 56. By contrast, the most common HPV types in CIN1 were HPV 58 (18.8%) and HPV 16/35 (18.8%) [15]. In the cross-sectional study in Norway, presence of HPV 16 as a single infection or in combination with another HPV genotype was more common in women with CIN3+ than in women with CIN2. Although less prevalent, HPV 33 was also more common in women with CIN3+ than in women with CIN2 [14]. In a pooled data analysis, including more than 16,000 women from different countries, HPV 16, 18, and 45 were more frequently reported in women with invasive carcinoma than in women with high-grade squamous intraepithelial lesions [16]. In our study, intermediate risk (HPV 31, 33, 35, 51, 52, and 58), high risk/HPV 16 and high risk/HPV 18 (HPV 18, 45, and 56) were significantly more common in women with CIN3+ than CIN1/CIN2.
The distribution of HPV genotypes and HPV genotypes by severity of CIN differs little between previous studies and our study. Inclusion of CIN1 in our study might have made some difference.
After treatment of CIN with LEEP, there is always a possibility of residual/recurrent or even new lesion. The resection margin status is a predictor of residual/recurrent disease. Involved resection margins suggest that the lesion has not been completely removed, i.e., that on the remaining part of the cervix there is still some lesion left. In a study including 1,062 patients treated for CIN2/CIN3 by carbon dioxide laser conization, involved resection margins were significantly associated with both residual and recurrent disease compared with disease-free resection margins as reference [7]. In another study including 172 patients who had undergone cervical conization followed by hysterectomy, patients with positive margins had significantly higher risks of having residual lesion than those with negative margins [17]. As for status of margin by HPV genotypes, we could not find any previous study. In our study, the proportion of positive margin was significantly different (P < 0.01) by HPV genotypes. It was highest in the high risk/HPV 18 group followed by the high risk/HPV 16, intermediate risk, unclassified and negative groups. HPV 18-related cervical carcinomas, particularly those diagnosed at an early stage, were associated with a poor prognosis [18]. In other studies, HPV 18 was a poor prognostic factor in patients with stage IB-IIA cervical cancer undergoing radical hysterectomy [19,20]. There is a thread of connection between our study and the previous studies.
In our study, we defined progression as abnormal cytology including ASC, LSIL, and HSIL. The large population of women with minimally abnormal cervical cytology needs accurate triage. A prospective study including 46,009 women showed that, of the total number of cases of histologically confirmed high-grade cervical neoplasia, the largest proportion (38.8%) was in women with smears showing ASC-US [21]. In 3,488 women with a community-based ASC-US, the 2-year cumulative diagnosis of CIN3 was 8% to 9% [22]. In another study including 278 patients with ASC-US, 11.9% of patients had CIN2 or CIN3 [23]. In 86 ASC-US cases with histologic follow-up, ASC-US, 5.8% of the patients had HSIL and one vulvar HSIL was detected [24]. We concluded that the risk for high grade lesion in ASC-US is not negligible and included ASC-US.
The margin status was the only statistically significant factor in our study. While the high risk/HPV 18 group had lower PFS than other groups, that difference could have occurred by chance. The median duration of the follow-up was 11 months, not long enough to adequately assess long-term survival. If the observation period were longer or our study sample larger, the high risk/HPV 18 group difference might prove significant.
Our study has some limitations. First, the resection range of the CIN lesion was not standardized because LEEP was performed by several gynecologists. Second, as mentioned above, the duration of the follow-up was not long. Third, HPV testing was not performed routinely at follow-up. So, we could not evaluate the effect of residual HPV infection on prognosis.
Despite these limitations, our study is, to the best of our knowledge, the first study that shows the different proportion of the positive margin by HPV genotypes in CIN patients treated with LEEP. In conclusion, our study shows that CIN patients with high risk/HPV 18 need to be more carefully tracked than patients with the other HPV genotypes.

 XML Download
XML Download