

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
This study was designed to compare the ultrasonographic features of papillary thyroid carcinoma with and without Hashimoto's thyroiditis.
Materials and Methods
This retrospective study included 190 patients with papillary thyroid carcinoma which was proven by neck surgery. The difference in the ultrasonographic findings between papillary thyroid carcinoma with Hashimoto's thyroiditis and papillary thyroid carcinoma without Hashimoto's thyroiditis were calculated statistically.
Results
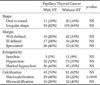
Hashimoto's thyroiditis was diagnosed in 61 of 190 patients following neck surgery. The incidence of coexisting papillary thyroid carcinoma with Hashimoto's thyroiditis was significantly higher in women (p=0.0026). In addition, the frequency of macrocalcification in patients with Hashimoto's thyroiditis was also significantly higher (p=0.0009). Conversely,other ultrasonographic findings including the shape, margin, echogenicity and calcifications, for patients with papillary thyroid carcinoma with Hashimoto's thyroiditis and papillary thyroid carcinoma without Hashimoto's thyroiditis, were not statistically significant. We also found that patients with Hashimoto's thyroiditis who showed no calcification on ultrasonography tended not to detect the papillary carcinoma at a higher frequency.
Conclusion
On ultrasonography, macrocalcifications occurred more frequently in patients with Hashimoto's thyroiditis than those without Hashimoto's thyroiditis. Malignant thyroid nodules without calcifications in patients with Hashimoto's thyroiditis more often could not be detected. Therefore, it is important carefully examine patients with Hashimoto's thyroiditis.
Figures and Tables
Fig. 1
A photomicrograph of Hashimoto's thyroiditis shows lymphocytes infiltration with germinal center formation (H & E, ×40).
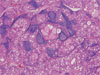
Fig. 2
US images of papillary thyroid carcinoma with Hashimoto's thyroiditis in a 55-year-old women.
A. Transverse US image shows ill defined multiple hypoechoic micronodules in thyroid gland.
B. A irregular shaped, and marked hypoechoic nodule with a macrocalcification (arrow).

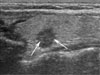
Fig. 3
Longitudinal US image of papillary thyroid carcinoma without Hashimoto's thyroiditis in a 41-year-old women shows a speculated, irregular shaped, and marked hypoechoic nodule with microcalcifications (arrows).

References
1. Hedinger C, Williams ED, Sobin LH. The WHO histological classification of thyroid tumors: a commentary on the second edition. Cancer. 1989; 63:908–911.
2. Hundahl SA, Fleming ID, Fremgen AM, Menck HR. A national cancer data base report on 53,856 cases of thyroid carcinoma treated in the U.S., 1985-1995 see commetns. Cancer. 1998; 83:2638–2648.
3. Takashima S, Matsuzuka F, Nagareda T, Tomiyama N, Kozuka T. Thyroid nodules associated with hashimoto thyroiditis: assessment with US. Radiology. 1992; 185:125–130.
4. Dailey ME, Lindsay S, Skahen R. Relation of thyroid neoplasms to hashimoto disease of the thyroid gland. AMA Arch Surg. 1955; 70:291–297.
5. Hirabayashi RN, Lindsay S. The relation of thyroid carcinoma and chronic thyroiditis. Surg Gynecol Obstet. 1965; 121:243–252.
6. Matsubayashi S, Kawai K, Matsumoto Y, Mukuta T, Morita T, Hirai K, et al. The correlation between papillary thyroid carcinoma and lymphocytic infiltration in the thyroid gland. J Clin Endocrinol Metab. 1995; 80:3421–3424.
7. Kurukahvecioglu O, Taneri F, Yuksel O, Aydin A, Tezel E, Onuk E. Total thyroidectomy for the treatment of hashimoto’s thyroiditis coexisting with papillary thyroid carcinoma. Adv Ther. 2007; 24:510–516.
8. Erdogan M, Erdem N, Cetinkalp S, Ozgen AG, Saygili F, Yilmaz C, et al. Demographic, clinical, laboratory, ultrasonographic, and cytological features of patients with hashimoto's thyroiditis: results of a university hospital of 769 patients in turkey. Endocrine. 2009; Forthcoming.
9. Moshynska OV, Saxena A. Clonal relationship between hashimoto thyroiditis and thyroid lymphoma. J Clin Pathol. 2008; 61:438–444.
10. Ohmori N, Miyakawa M, Ohmori K, Takano K. Ultrasonographic findings of papillary thyroid carcinoma with hashimoto’s thyroiditis. Intern Med. 2007; 46:547–550.
11. Yeh HC, Futterweit W, Gilbert P. Micronodulation: ultrasonographic sign of hashimoto thyroiditis. J Ultrasound Med. 1996; 15:813–819.
12. Simeone JF, Daniels GH, Mueller PR, Maloof F, vanSonnenberg E, Hall DA, et al. High-resolution real-time sonography of the thyroid. Radiology. 1982; 145:431–435.
13. Gul K, Ersoy R, Dirikoc A, Korukluoglu B, Ersoy PE, Aydin R, et al. Ultrasonographic evaluation of thyroid nodules: comparison of ultrasonographic, cytological, and histopathological findings. Endocrine. 2009; Forthcoming.
14. Moon W, Jung SL, Lee JH, Na DG, Baek J, Lee YH, et al. Benign and malignant thyroid nodules: US differentiation-multicenter retrospective study. Radiology. 2008; 247:762–770.
15. Wienke JR, Chong WK, Fielding JR, Zou KH, Mittelstaedt CA. Sonographic features of benign thyroid nodules: interobserver reliability and overlap with malignancy. J Ultrasound Med. 2003; 22:1027–1031.
16. Taki S, Terahata S, Yamashita R, Kinuya K, Nobata K, Kakuda K, et al. Thyroid calcifications: sonographic patterns and incidence of cancer. Clin Imaging. 2004; 28:368–371.
17. Kim E, Park CS, Chung WY, Oh KK, Kim DI, Lee JT, et al. New sonographic criteria for recommending fine-needle aspiration biopsy of nonpalpable solid nodules of the thyroid. AJR Am J Roentgenol. 2002; 178:687–691.
18. Takashima S, Fukuda H, Nomura N, Kishimoto H, Kim T, Kobayashi T. Thyroid nodules: re-evaluation with ultrasound. J Clin Ultrasound. 1995; 23:179–184.
19. Tessler F, Tublin M. Thyroid sonography: current applications and future directions. AJR Am J Roentgenol. 1999; 173:437–443.
20. Frates MC, Benson CB, Charboneau JW, Cibas ES, Clark OH, Coleman BG, et al. Management of thyroid nodules detected at US: Society of Radiologists in Ultrasound consensus conference Statement. Radiology. 2005; 237:794–800.
21. Wirtschafter A, Schmidt R, Rosen D, Kundu N, Santoro M, Fusco A, et al. Expression of the RET/PTC fusion gene as a marker for papillary carcinoma in hashimoto’s thyroiditis. Laryngoscope. 1997; 107:95–100.
22. Tamimi DM. The association between chronic lymphocytic thyroiditis and thyroid tumors. Int J Surg Pathol. 2002; 10:141–146.
23. Schaffler A, Palitzsch KD, Seiffarth C, Hohne HM, Riedhammer FJ, Hofstadter F, et al. Coexistent thyroiditis is associated with lower tumour stage in thyroid carcinoma. Eur J Clin Invest. 1998; 28:838–844.
24. Kebebew E, Treseler PA, Ituarte PH, Clark OH. Coexisting chronic lymphocytic thyroiditis and papillary thyroid cancer revisited. World J Surg. 2001; 25:632–637.
25. Matesa-Anic D, Matesa N, Dabelic N, Kusic Z. Coexistence of papillary carcinoma and hashimoto’s thyroiditis. Acta Clin Croat. 2009; 48:9–12.
26. Kashima K, Yokoyama S, Noguchi S, Murakami N, Yamashita H, Watanabe S, et al. Chronic thyroiditis as a favorable prognostic factor in papillary thyroid carcinoma. Thyroid. 1998; 8:197–202.
27. Kim EY, Kim WG, Kim WB, Kim TY, Kim JM, Ryu JS, et al. Coexistence of chronic lymphocytic thyroiditis is associated with lower recurrence rates in patients with papillary thyroid carcinoma. Clin Endocrinol (Oxf). 2009; 71:581–558.
28. Loh KC, Greenspan FS, Dong F, Miller TR, Yeo PP. Influence of lymphocytic thyroiditis on the prognostic outcome of patients with papillary thyroid carcinoma. J Clin Endocrinol Metab. 1999; 84:458–463.
 XML Download
XML Download