

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Intracranial epidermoid cysts have been reported to make up less than 2% of all intracranial space-occupying lesions (1). They are most commonly located in the cerebellopontine angle cistern, which accounts for approximately 40-50% of all intracranial epidermoid cysts, and this is followed by the parasellar region. Epidermoid cysts involving the cavernous sinus are very rare and they can be divided into 3 categories according to their location; extracavernous, interdural and true intracavernous (2). Herein we present the CT and MR imaging features, including the precontrast CT, fluid-attenuated inversion recovery (FLAIR), diffusion-weighted (DW) and constructive interference in steady state (CISS) images, of an unusual case of a true, pathologically proven intracavernous epidermoid cyst.
Case Report
A 22-year-old male presented with progressed ophthalmoplegia. He was diagnosed with a mass in the right cavernous sinus 3 years previously and he underwent gamma knife radiosurgery at an outside clinic. But the size of the mass didn't decrease and instead, his symptoms were aggravated. On the neurologic examination, he presented with right lateral gaze paralysis, diplopia and right fascial paresthesia of the maxillary nerve area.
The initial precontrast CT scan demonstrated a well-defined contour-bulging oval shaped cystic mass in the right cavernous sinus. A focal indistinct round hyperattenuated portion was seen at the anterior portion of the mass (Fig. 1A). We obtained the brain MR images for further evaluation. The mass was mostly hypointense on the T1-weighted MR images (Fig. 1B) and slightly heterogeneous hyperintense on the T2-weighted MR images (Fig. 1C). The anterior focal hyperattenuated portion on the CT scan was hyperintense on the T1-weighted MR images and hypointense on the T2-weighted MR images (arrowhead in Figs. 1B, C). On the gadolinium-enhanced T1 weighted MR images, the mass did not show contrast enhancement (Fig. 1D). The thicker lateral margin of the mass was seen as a dark signal rim on the T2-weighted images. The coronal T2-weighted images showed dark signal intensities in the lateral wall of the right cavernous sinus, and this suggested that the cranial nerves were laterally displaced by the mass (Fig. 1E). The heterogeneous signal intensity on the T2-weighted images was well demonstrated on the FLAIR images (Fig. 1F) and CISS images (Fig. 1G). The DWI showed restricted diffusion in most parts of the mass, and this was seen as bright high signal intensity (Fig. 1H). A cavernous segment of the right internal carotid artery (ICA) was displaced anteromedially. Dural reflection of the lateral wall was clearly seen on the T2-weighted SE and CISS images.
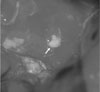
On the operation field, the lateral wall of the right cavernous sinus was thickened and adhered to the adjacent dura, so it was difficult to identify the cranial nerves and finally, the 6th nerve was not precisely identified. After incision of the dura of the lateral wall, a pearly white mass was seen (Fig. 2). The entire tumor was located within the right cavernous sinus (a pure intracavernous sinus location). We totally resected the mass.
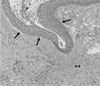
Histologic examination showed a cystic mass with a typical stratified squamous epithelial lining, keratin and adjacent nerve sheaths (Fig. 3).
After surgery, the patient's symptoms of right fascial paresthesia and upward gaze paralysis were completely improved, but the lateral gaze paralysis was sustained. He was discharged after 2 weeks without any additional neurologic deficit.
Discussion
Epidermoid cysts arise from ectodermal inclusion during the time of neural tube closure at between the 3rd to 5th weeks of embryonic development. Intracranial locations are rare, and but the reported locations have included the cerebral interhemispheres, the lateral ventricle and the brain stem (345). Epidermoid cysts involving the cavernous sinus are very rare. Gharabaghi et al. (2) classified epidermoid cysts involving the cavernous sinus into 3 categories by according to their location: extracavernous, interdural and true intracavernous. There are only rare reports of true intracavernous epidermoid cysts (2678) and there are no reports about the MR findings, including the DW, FLAIR and CISS images.
Primary tumors originating within the cavernous sinus are rare. The tumors in the cavernous sinus are mostly meningioma, neurogenic tumors (schwannoma, neurofibroma) and cavernous hemangioma. But these tumors are usually well-enhancing solid masses. If a mass in the cavernous sinus has a cystic portion, then we should consider cystic schwannoma, arachnoid cyst or epidermoid cyst.
Epidemoid cysts show characteristic signal intensity as isointense or slightly hyperintense relative to the CSF signal on the T1-weighted images and they are similarly hyperintense relative to the CSF signal on the T2-weighted images. However, unlike the homogeneously hyperintense signal of the CSF, epidermoid cysts have a slightly heterogeneous appearance on T2-weighted images. Because the cystic mass is not completely suppressed on FLAIR images, the mass is more heterogeneous in signal intensity. The CISS sequence provides high resolution images with good contrast between the CSF and solid structures. Restricted diffusion with high signal intensity is characteristically shown on the DW images. Most epidermoid cysts do not enhance, although some minimal rim enhancement occurs in approximately 25% of cases.
In our case, the lateral wall of the right cavernous sinus was thickened and adhered to the adjacent dura, and we thought this was probably the result of previous gamma knife radiosurgery. The coronal T2-weighted MR images showed a thickened lateral wall of the right cavernous sinus with a portion of dot-like dark signal intensity, and this was suggestive of the areas corresponding to the displaced cranial nerves. The displacement of the cranial nerves was a clue for the location of the mass as an intracavernous location, and not an interdural or parasellar location.
On CT scans, most epidermoid cysts typically appear as non-enhancing hypoattenuated lesions. Calcification is present in 10-25% of cases (3). Rare "white" or "dense" epidermoid cysts have a high level of proteineous content and these rare cysts may appear as hyperattenuated lesion on CT scan (9). These "white" or "dense" cysts are filled with soft, waxy or flaky keratohyalin material that comes about from progressive desquamation of the cyst wall. On microscopic examination, the lining cells of epidermoid cyst consist of stratified squamous epithelium supported by an outer layer of collagenous connective tissue. The cystic contents usually include debris, keratin, water, and cholesterol laid down in a lamellar fashion (10).
In conclusion, making an exact diagnosis of epidermoid cysts within the true cavernous sinus is essential for deciding on therapy, such as microsurgery or radiation therapy. If a cystic mass involving the cavernous sinus is found, then the radiologist should recommend MR imaging, including the DWI and CISS sequences or others. High signal intensity on the DWIs is a characteristic diagnostic feature of epidermoid cyst. The CISS sequence is useful to reveal the detailed relationships between the dural wall and the cranial nerves. The presence of dural reflection in the lateral wall of the cavernous sinus and displacement of the cranial nerves laterally and the intracavernous ICA medially are clues of an intracavernous location of epidermoid cyst.

 XML Download
XML Download