

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Remarkable advances have occurred in recent years in understanding the molecular biology of thyroid cancer. Various somatic mutations associated with the development and progression of thyroid carcinomas have been discovered [1,2,3,4]. Our rapidly expanding knowledge of the molecular genetics of thyroid cancer has shifted into clinical practice, offering better diagnostic accuracy and enabling the development of novel compounds for the treatment of advanced metastatic thyroid carcinoma [5,6,7,8]. As the most common and challenging problem in thyroid carcinoma is related to the diagnosis and prognostication of well-differentiated thyroid cancer (WDTC), this review will focus on the genetic abnormalities found in WDTC and their diagnostic and prognostic use, as well as on therapies targeted to specific mutated sites and kinase pathways.
PROTO-ONCOGENES COMMONLY ASSOCIATED WITH WELL-DIFFERENTIATED THYROID CARCINOMA
Chromosomal rearrangements (RET/PTC)
The rearranged during transfection (RET) proto-oncogene is located on chromosome 10q11-12 and encodes a transmembrane receptor with a tyrosine kinase domain. Because it was first found only in papillary thyroid cancer (PTC), it is called RET/PTC [9]. Although more than ten rearrangements have been identified, RET/PTC1 and RET/PTC3 account for most of the rearrangements found in PTC [10]. The RET/PTC chimeric oncogenic protein leads to the activation of several downstream pathways, including mitogen-activated protein kinase (MAPK), extracellular signal-related kinase (ERK), and phosphatidylinositol 3-kinase (PI3K). The prevalence of RET/PTC rearrangements in sporadic papillary carcinoma is approximately 15% to 40% [11]. The RET/PTC rearrangement has also been detected in the follicular variant of PTC (FVPTC) [9]. Clinically, RET/PTC variants are often found in radiation-associated PTC. Following the Chernobyl nuclear plant explosion in 1986, there was an increase in pediatric PTC and an increase in the incidence of an aggressive solid variant of PTC that contained the RET/PTC3 rearrangement. A form of PTC with a later onset, with a more classical phenotype and clinical course, emerged in the Chernobyl survivors and contained RET/PTC1 [12].
RAS mutations
The Rat sarcoma (RAS) oncogene families regulate two important signaling pathways in thyroid cancer, the MAP kinase cascade (Ras-Raf-MEK-ERK) and the PI3K/Akt signaling pathway. Mutations of H-RAS codon 61 and N-RAS codon 61 are the most common RAS mutations associated with thyroid cancer [13]. RAS mutations occur in both benign tumors and thyroid cancers (both PTC and follicular thyroid cancer [FTC]), with variable frequency in anaplastic thyroid cancers. PTC with RAS mutations often display a follicular architecture and are called FVPTC. PTCs carrying a RAS mutation tend to exhibit a lower rate of lymph node metastasis and are more likely to be encapsulated [14].
BRAF and the MAP kinase pathway
The MAP kinase pathway mediates cellular responses to growth signals [4]. The MAPK pathway consists of a three-tiered protein kinase cascade: an extracellular signal (growth factor) interacts with a receptor tyrosine kinase, which then stimulates the activity of a MAPK kinase kinase (a MAPKKK, e.g., Raf) via the G-protein Ras, which activates a MAPKK (e.g., MEK), which in turn activates a MAPK (e.g., ERK). ERK is able to phosphorylate a number of proteins that regulate cytoskeletal organization, metabolism, chromatin remodeling, and numerous transcription factors (Fig. 1). There are three kinds of Raf proteins: A-Raf, B-Raf, and C-Raf (or Raf-1). Activation of B-Raf occurs after binding to Ras alone, whereas for activation of A-Raf and C-Raf, additional signals are required [15]. B-Raf is therefore the most potent activator of downstream effector MEK kinases in the Raf-Raf-MEK-ERK pathway. Mutations in the MAP kinase pathway are found in approximately 30% of all cancers, while around 8% of cancers develop due to BRAF mutations [16,17].
BRAF mutations were first discovered in thyroid cancer in 2003 [1]. A missense mutation in exon 15, which occurs due to the substitution of the amino acid valine for glutamic acid at residue position 600 [16], is present in 36% to 69% of PTC cases and is the most frequent genetic change in PTC [18,19]. The V600E mutation comprises more than 90% of observed BRAF mutations. In subtypes of PTC, the highest rate of BRAF mutation (77%) is found in the tall cell variant of papillary cancer, and the lowest percentage (12%) is found in the FVPTC. In PTC, BRAF mutation is more frequent in older patients, and is associated with extrathyroidal invasion, advanced stage, and worse clinical outcome, including greater rates of recurrence and treatment failure [20,21,22,23]. BRAF mutation is responsible for the suppression of the sodium/iodide symporter (NIS), which is involved in iodine metabolism [24]. By contrast, others have found that the BRAF mutation is not associated with age, gender, multicentricity, recurrence rate, lymphovascular invasion, extranodal extension, central neck involvement, advanced stage (stage III or IV), or distant metastasis [25,26,27].
PAX8/PPAR
The most common genetic abnormalities involved in follicular thyroid carcinoma are deletions, partial deletions, and deletion rearrangements of the short arm of chromosome 3. The PAX8/PPAR fusion oncogene occurs via a balanced translocation between chromosomes 2 and 3 that results in the fusion of the DNA-binding domains of the thyroid transcription factor PAX8 to the peroxisome proliferator activated receptor (PPARγ) [3]. The PAX8/PPAR fusion protein (PPFP) is detected in 36.5% of FTCs (range, 11% to 63%), 9.5% of follicular adenomas, and 13.2% of FVPTCs [28]. This chimeric protein may retard the growth inhibition and follicular differentiation normally induced by PPARγ, resulting in tumorigenesis. PPFP is not the only PPARγ fusion mutation that occurs in FTC. Recently, the CREB3L2-PPARγ fusion, which results from a t(3;7)(p25;q34) chromosomal rearrangement, was identified [29].
TARGETED THERAPIES
The treatment of patients with well-differentiated thyroid carcinoma is based on surgery, high-dose radioactive iodine (RAI), and thyroid hormone therapy. However, for patients with advanced, metastatic thyroid carcinoma, treatment options after radioiodine and thyroid hormone therapy have been limited. In patients with radioiodine-resistant disease, cytotoxic chemotherapy yields low response rates of short duration, is often associated with considerable toxicity, and does not prolong survival.
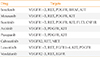
Recently, antiangiogenic therapy has been investigated for the treatment of advanced thyroid cancer. Investigational targeted therapies for WDTC include agents targeting the VEGF pathway and those targeting multiple kinases such as the MAP kinase and PI3 kinase pathways (Table 1) [6]. These inhibitors are typically administered orally and, because of the targeting similarities, common toxicities exist among these agents, including hypertension, diarrhea, skin rashes, and fatigue.
Sorafenib
Sorafenib is an oral tyrosine kinase inhibitor (TKI) targeting B-Raf and VEGF receptors 2 and 3. The optimal therapeutic dose of sorafenib is 400 mg twice daily [5]. In a phase II trial, 58 WDTC patients with RAI failure were treated with sorafenib over a 10-month period. Of 41 PTC patients, six had a partial response (PR) and 23 had stable disease lasting longer than 6 months. The median duration of the PR was 7.5 months, the median progression-free survival (PFS) was 15 months, and the thyroglobulin of 77% of PTC patients declined more than 25%. No PRs were noted among non-PTC patients [30]. Another phase II study evaluated the effect of 26 weeks of sorafenib therapy on 31 WDTC patients with metastatic or locally advanced, radioiodine-refractory disease. At the study end, 25% of patients had a PR, 34% had stable disease, and the PFS was 58 weeks. Of 21 patients who underwent radioiodine imaging after 26 weeks of treatment, none had induction of uptake in metastatic lesions [7].
Motesanib
Motesanib is also an oral TKI targeting VEGF receptors 1, 2, and 3. In an open-label, phase II study, 57 PTC patients who had progressive, locally advanced or metastatic, radioiodine-resistant WDTC were treated with 125 mg of motesanib administered orally once daily. The objective response rate was 14%, and stable disease was achieved in 67% of the patients and maintained for 24 weeks or longer in 35%. The median duration of the response was 32 weeks and the median PFS was 40 weeks. Serum thyroglobulin concentrations decreased during treatment in 81% of patients [31].
Sunitinib
Sunitinib is approved for the treatment of renal cell carcinoma and is a TKI targeting all three VEGF receptors, RET, and RET/PTC subtypes 1 and 3. Prolonged PRs have been described in three patients (with PTC, FTC, and MTC, respectively) treated with 50 mg of sunitinib daily for 28 days followed by 14 days without treatment per cycle. Fluoro-2-deoxy-D-glucose uptake by positron emission tomography imaging was markedly reduced in the WDTC patients [32]. An open-label phase II trial with sunitinib in 35 patients with progressive WDTC or MTC reported a PR in 13% of 31 WDTC patients, and disease stabilization in 68% of WDTC and 83% of MTC patients [33].
Axitinib and pazopanib
Although the above TKIs targeting the VEGF receptors also inhibit RET, axitinib, and pazopanib do not have any anti-RET activity [34,35]. Axitinib and pazopanib are efficacious in thyroid carcinoma despite the absence of inhibitory activity against RET or other mutated kinases that are oncogenic in thyroid carcinoma, suggesting that VEGF receptor-mediated angiogenesis is likely the primary mechanism by which the other anti-VEGF receptor inhibitory agents function.
Thalidomide
Thalidomide was found to inhibit angiogenesis, but the exact mechanism by which thalidomide exerts its antiangiogenic effects remains unknown. An open-label, phase II trial was initiated to examine the efficacy of thalidomide in 36 patients with progressive, metastatic thyroid carcinoma [36]. Starting at 200 mg daily, the dose of thalidomide was progressively increased as tolerated, with a median maximum daily dose of 600 mg. PRs were achieved in 18% of patients, and 32% had stable disease as their best response. Common adverse events included somnolence, peripheral neuropathy, constipation, dizziness, and infection.
Celecoxib
Cyclooxygenase-2 (COX-2) is overexpressed in many cancers and promotes tumor development and progression. COX-2 mRNA and protein levels are increased in thyroid cancer compared with nonneoplastic and benign thyroid tissues, especially those expressing RET/PTC mutations. One phase II trial was performed in 32 patients with progressive WDTC treated with celecoxib 400 mg orally twice a day for 12 months. One patient had a PR, and one remained stable on therapy for >12 months, but most patients progressed despite treatment. The study was terminated as a result of a lack of efficacy combined with increasing concern about cardiovascular toxicity from COX-2 inhibitors [37].
Rosiglitazone
Rosiglitazone, a PPARγ agonist, has been shown to induce differentiation, cell cycle arrest, and apoptosis in a variety of human cancers, including thyroid carcinoma. Ten patients with radioiodine scan-negative metastatic WDTC were treated with rosiglitazone at 4 mg daily for 1 week, and then 8 mg daily for 7 weeks. Of the ten patients, four had positive radioiodine scans after rosiglitazone therapy, with uptake in the neck in three patients and in the pelvis in one patient. The serum thyroglobulin level decreased in two patients, increased in five patients, and was stable in three patients. No patient developed clinically important toxicity associated with rosiglitazone treatment.
CONCLUSIONS
Papillary thyroid carcinomas, follicular thyroid carcinomas, and their subtypes represent the majority of WDTCs. Mutations in RET/PTC, BRAF, RAS, and PAX8/PPARγ are commonly associated with well-differentiated thyroid carcinoma and may carry diagnostic and prognostic significance. These molecular markers are reflected in the Revised Management Guidelines for Patients with Thyroid Nodules and Differentiated Thyroid Cancer, published by the American Thyroid Association [38]. VEGF- and RET-directed therapies such as sorafenib, motesanib, and sunitinib, novel therapeutic agents targeting the above genetic mutations, have been shown to be the most effective at inducing clinical responses and stabilizing the disease process. In the near future, targeted therapy and the use of tumor biomarkers for predicting responses will be the next step in improving the survival of a disease that not long ago was untreatable.

 XML Download
XML Download