

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Developing Cushing's syndrome during pregnancy is rare because menstruation is irregular and hypercortisolism causes infertility. Developing Cushing's disease during pregnancy is very rare because there is even less ovulation than those with the adrenal adenoma. The clinical manifestations of Cushing's syndrome may easily be missed during pregnancy as the features of weight gain, hypertension, and hyperglycemia overlap with those that occur during a pregnancy. Diagnosing Cushing's syndrome during a pregnancy is complex because the biochemical features are obscured by the natural changes in the hypothalamic-pituitary-adrenal axis that occur during pregnancy. Having Cushing's syndrome during a pregnancy results in increased fetal and maternal complications, so early diagnosis and treatment are critical. We report the clinical and endocrine findings of a pregnant women with Cushing's disease who underwent transsphenoidal surgery after delivery.
Figures and Tables
Fig. 1
T1 noncontrast magnetic resonance imaging of sagittal (A) and coronal (B) views of a 1.3 cm complicated cystic mass at the sellar floor.
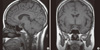
Fig. 2
Abdomen magnetic resonance imaging shows simple cyst in the right kidney, otherwise there is no remarkable findings in the both adrenal glands.
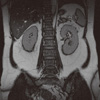
Fig. 3
T1 noncontrast magnetic resonance imaging of sagittal (A) and coronal (B) views show increased size of complicated cystic mass at the sellar floor.
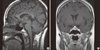
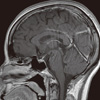
Fig. 4
A. Histological examination of the operative specimen showed pituitary adenoma with near total necrosis (H&E stain, × 40). B. Immunohistochemical stains were positive for adrenocortical hormone (immunohistochemistry ACTH, × 100).


References
1. Kita M, Sakalidou M, Saratzis A, Ioannis S, Avramidis A. Cushing's syndrome in pregnancy: report of a case and review of the literature. Hormones (Athens). 2007. 6:242–246.
2. Pickard J, Jochen AL, Sadur CN, Hofeldt FD. Cushing's syndrome in pregnancy. Obstet Gynecol Surv. 1990. 45:87–93.
3. Lindsay JR, Nieman LK. The hypothalamic-pituitary-adrenal axis in pregnancy: challenges in disease detection and treatment. Endocr Rev. 2005. 26:775–799.
4. Fayol L, Masson P, Millet V, Simeoni U. Cushing's syndrome in pregnancy and neonatal hypertrophic obstructive cardiomyopathy. Acta Paediatr. 2004. 93:1400–1402.
5. Sheeler LR. Cushing's syndrome and pregnancy. Endocrinol Metab Clin North Am. 1994. 23:619–627.
6. Hunt AB, McConahey WM. Pregnancy associated with diseases of the adrenal glands. Am J Obstet Gynecol. 1953. 66:970–987.
7. Lado-Abeal J, Rodriguez-Arnao J, Newell-Price JD, Perry LA, Grossman AB, Besser GM, Trainer PJ. Menstrual abnormalities in women with Cushing's disease are correlated with hypercortisolemia rather than raised circulating androgen levels. J Clin Endocrinol Metab. 1998. 83:3083–3088.
8. Yoo HJ, Ihm SH, Park SW, Yim HS, Kim YT, Park CH, Kim HK, Kim DM, Yoo JM, Choi MK. A case of Cushing's syndrome in pregnancy due to adrenal adenoma. J Korean Soc Endocrinol. 1998. 13:264–270.
9. Kim JG, Choo JS, Lee YK, Han BC, Jin SB, Yang SG, Song CS, Sin MG. A case of adrenal adenoma associated with pregnancy. J Korean Soc Endocrinol. 1994. 9:39–45.
10. Song KS, Hwang JK, Ju KT, Lee HJ, Song SH, Lee KY, Suh CJ, Kim HK, Park HY, Yang DM, Oh YH, Kang MH. A case of adrenalectomy after preterm delivery in Cushing's syndrome of third trimester pregnant woman. J Korean Soc Endocrinol. 2001. 16:134–139.
11. Lindholm J, Schultz-Möller N. Plasma and urinary cortisol in pregnancy and during estrogen-gestagen treatment. Scand J Clin Lab Invest. 1973. 31:119–122.
12. Chico A, Manzanares JM, Halperin I, Martínez de Osaba MJ, Adelantado J, Webb SM. Cushing's disease and pregnancy: report of six cases. Eur J Obstet Gynecol Reprod Biol. 1996. 64:143–146.
13. Invitti C, Pecori Giraldi F, de Martin M, Cavagnini F. Study Group of the Italian Society of Endocrinology on the Pathophysiology of the Hypothalamic-Pituitary-Adrenal Axis. Diagnosis and management of Cushing's syndrome: results of an Italian multicentre study. J Clin Endocrinol Metab. 1999. 84:440–448.
14. Nolten WE, Lindheimer MD, Rueckert PA, Oparil S, Ehrlich EN. Diurnal patterns and regulation of cortisol secretion in pregnancy. J Clin Endocrinol Metab. 1980. 51:466–472.
15. Newell-Price J, Trainer P, Besser M, Grossman A. The diagnosis and differential diagnosis of Cushing's syndrome and pseudo-Cushing's states. Endocr Rev. 1998. 19:647–672.
16. Magiakou MA, Mastorakos G, Rabin D, Margioris AN, Dubbert B, Calogero AE, Tsigos C, Munson PJ, Chrousos GP. The maternal hypothalamic-pituitary-adrenal axis in the third trimester of human pregnancy. Clin Endocrinol (Oxf). 1996. 44:419–428.
17. Aron DC, Raff H, Findling JW. Effectiveness versus efficacy: the limited value in clinical practice of high dose dexamethasone suppression testing in the differential diagnosis of adrenocorticotropin-dependent Cushing's syndrome. J Clin Endocrinol Metab. 1997. 82:1780–1785.
18. Oh HC, Koh JM, Kim MS, Park JY, Shong YK, Lee KU, Kim GS, Hong SJ, Koo HL, Kim WB. A case of ACTH-producing pheochromocytoma associated with pregnancy. Endocr J. 2003. 50:739–744.
19. Lindsay JR, Jonklaas J, Oldfield EH, Nieman LK. Cushing's syndrome during pregnancy: personal experience and review of the literature. J Clin Endocrinol Metab. 2005. 90:3077–3083.
20. Mellor A, Harvey RD, Pobereskin LH, Sneyd JR. Cushing's disease treated by trans-sphenoidal selective adenomectomy in mid-pregnancy. Br J Anaesth. 1998. 80:850–852.
 XML Download
XML Download