

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
For patients with locally advanced cervical cancer (LACC), the current guidelines recommend primary chemoradiotherapy (CRT) [1]. Therefore, pre-therapeutic staging has an important role in the management of patients with LACC. Assessment of the nodal involvement of para-aortic lymph nodes (PALN) is critical to determine the field of radiation therapy (RT).
The value of pre-treatment surgical PALN assessment has been evaluated in previous studies; however, the survival benefit of surgical staging has not yet been determined. One randomized trial failed to show any benefit of surgical staging [2]. This trial was stopped prematurely after an interim analysis owing to a significant reduction in survival for patients staged surgically. Conversely, surgical staging has been shown to improve survival compared to conventional radiological staging in three Gynecologic Oncology Group (GOG) trials (GOG 85, GOG 120, and GOG 165) [3]. Recently, a Cochrane review concluded that the decision to offer pre-treatment surgical PALN assessment needs to be individualized in LACC [4].
In the era of positron emission tomography/computed tomography (PET/CT), the role of surgical staging should be re-evaluated. PET/CT is the most accurate imaging method for assessing extrapelvic disease in LACC [5]. Its high true-positive rate for PALN metastasis suggests that surgical staging is unnecessary when uptake is noted in the paraaortic area. However, the overall false-negative rate of PALN involvement is around 12%, most of which is attributable to non-detectable nodal disease [6]. As such, surgical staging is potentially beneficial for patients who test negative for PALN on PET/CT. Considering postoperative complications and the high cost of surgical staging, a comprehensive cost-effective analysis is required to clarify the best treatment strategy for patients with LACC [47].
We sought to create a model to evaluate the cost-effectiveness of nodal staging surgery followed by tailored CRT compared to pelvic CRT for the treatment of LACC when no uptake is found in PALN on PET/CT.
MATERIALS AND METHODS
A modified Markov model was constructed using TreeAge Pro software (TreeAge Software Inc., Williamstown, MA, USA). The model evaluated two strategies for patients with stage IIB or higher disease that were scheduled to undergo CRT for curative intent when no uptake was recorded in PALN on PET/CT (Fig. 1). The strategies were (1) pelvic CRT in line with PET/CT results and (2) nodal staging surgery, followed by extended-field CRT if PALN metastasis was found and pelvic CRT otherwise. The Markov states were (1) active treatment; (2) completed primary treatment without complications; (3) completed primary treatment with acute complications; (4) completed primary treatment with late complications; and (5) death. The cycle length was 1 year, and the time horizon for the analysis was 5 years.
Under strategy 1, all patients were assumed to receive whole pelvic external-beam radiation (WPRT), six cycles of platinum-based chemotherapy, and additional vaginal cylinder brachytherapy regardless of PALN status. Under strategy 2, all patients were assumed to receive PALN dissection up to renal vessel level followed by definite CRT; if PALN metastasis was found following surgery, extended-field RT, six cycles of platinum-based chemotherapy, and additional brachytherapy would be performed; if no metastasis was found in the PALN, patients would undergo WPRT, six cycles of platinum-based chemotherapy, and brachytherapy. The baseline model was developed from a payer's perspective. Costs included hospital and professional costs associated with surgery, CRT, treatment of toxicity, and complications. Institutional Review Board approval was waived in this cost-effectiveness analysis due to using datasets open to the public.
2. Survival
Survival data were extracted from the literature. We categorized three cohorts to estimate outcomes: cohort 1, patients who undergo pelvic CRT without PALN metastasis; cohort 2, patients who undergo pelvic CRT only, despite the presence of occult PALN metastasis (unstaged PALN metastasis); and cohort 3, patients who undergo extended-field CRT due to PALN metastasis (fully staged PALN metastasis). Strategy 1 included the outcomes of cohorts 1 and 2, while strategy 2 included the outcomes of cohorts 1 and 3.
For patients receiving pelvic CRT in the setting of no PALN involvement, 5-year overall survival was estimated based on the published literature [891011]. Survival for individuals with occult PALN metastasis treated with extended-field CRT (cohort 3) was similar to that for patients without PALN metastasis and whose disease was managed with pelvic CRT alone (cohort 1) [1213]. As no survival data were available for patients who receive pelvic CRT only, despite the presence of PALN metastasis (cohort 2), this assumption was varied in the sensitivity analysis to correct for the uncertainty in the assumption. Five-year overall survival for patients with unstaged PALN metastasis (cohort 2) was modeled at 45%, reflecting a 30% reduction in survival compared to nodal staging surgery followed by extended-field CRT in occult PALN metastasis (cohort 3). Considering the 12% baseline false-negative rate for PET/CT in detecting PALN metastasis, strategy 1 included 88% of cohort 1 and 12% of cohort 2, and strategy 2 consisted of 88% of cohort 1 and 12% of cohort 3. Assuming that the survival rate in cohort 2 was 30% less than that in cohort 3, we could infer that the 5-year overall survival rate for patients in strategy 2 was approximately 2.4% higher than that of patients in strategy 1 in terms of baseline PET/CT performance.
3. Utilities
Quality of life (QOL) adjustments are listed in Table 1. We also assumed same utility conditions as suggested in a previous study [14]. QOL during the treatment phase was estimated at 0.76 [15]. For the 3 months of recovery from radiotherapy (RT), utility was assumed to be 0.86 [16]. Loss in QOL from acute gastrointestinal (GI) complications was based on toxicity for grade 3 to 4 nausea/vomiting/anorexia and diarrhea or proctitis [1718]. Acute genitourinary (GU) QOL was estimated based on the utility value for cystitis [19]. Patient QOL from chronic GI and GU toxicities was based on utilities for bowel obstruction and rectovaginal/vesicovaginal fistula [20]. Upon completion of active treatment, patients were assumed to return to a cervical cancer survivor utility score for Korea (0.898) unless they experienced late complications, in which case the appropriate utility score was then applied [21].
4. Toxicity
We assumed the same toxicity conditions as suggested in a previous study [14]. In this study, toxicity was based on conventional RT technology. Baseline probability estimates are shown in Table 1. Acute GI toxicities include nausea/vomiting/anorexia and diarrhea or proctitis. Bowel obstruction was included as a chronic GI condition. Acute GU toxicities included cystitis, and chronic GU conditions were rectovaginal and vesicovaginal fistulas.
5. Cost
Costs were incorporated into the model using claims data from the Health Insurance Review and Assessment Service (Table 2). Amounts are expressed in US dollars; the exchange rate was 1,121.00 Korean won to one US dollar in July 2013. A payer perspective was used.
Costs excluding complications were investigated using microcosting, which calculates costs after listing the total resources used and matching the unit cost of each component. Nodal staging surgery costs included fees for laparoscopic surgery, pathology, anesthesia, and 4 days of admission. Since intensity-modulated RT was not commonly used in Korea at that time, its associated cost was not included in this model. Chemotherapy costs were calculated for a hypothetical woman with a body surface area of 1.5 m2 and included the cost of administration, pre-medication, and the chemotherapeutic agent. The calculated dose for the chemotherapy regimen was cisplatin at 40 mg/m2. For complications, patient-level costs were collected and the average cost calculated. All patients were assumed to incur the cost of cancer treatment, excluding palliative care, when entering the first Markov cycle. Costs attributed to the final year of life were obtained from a retrospective assessment of Korean health-care costs attributed to the last year of life in patients with terminal cervical cancer [22].
6. Key assumptions
Key assumptions of our study are as follows: (1) all surgical staging is performed using an extraperitoneal laparoscopic approach, and nodal staging surgery is 100% sensitive and specific; (2) if PET/CT shows negative findings in PALN, occult nodal metastases (unstaged PALN) measure less than 5 mm at the time of surgical staging; and (3) definite CRT is performed within 4 weeks of nodal staging surgery and no damage results from a delay in starting curative treatment. In addition, we do not consider other postoperative complications, with the exception of lymphoceles and lymphedema, as the incidence of these complications is very low if a highly skilled surgeon performs the operation using an extraperitoneal approach.
7. Cost-effectiveness and sensitivity analysis
Effectiveness was calculated in quality-adjusted life years (QALY). Costs are discounted at 5% annually. The incremental cost-effectiveness ratio (ICER) is the ratio of the additional economic impact of a strategy relative to the improvement in QALY.
We conducted one-way sensitivity and probabilistic sensitivity analyses to evaluate the impact of a variation in parameters on the resulting ICER. One-way sensitivity analyses were carried out based on the performance of PET/CT (false-negative rates), rates of postoperative complications, and survival reduction when pelvic CRT alone was performed for patients with unstaged PALN metastasis. To quantify the comprehensive effect of uncertainty, a probabilistic sensitivity analysis was tested using a Monte Carlo simulation.
RESULTS
1. Base case
In the base-case analysis, with a 12% false-negative rate of PET/CT detecting PALN metastasis, nodal staging surgery followed by tailored CRT resulted in an additional cost of $921 per patient, with an increase in effectiveness of 0.048 QALYs. Compared to pelvic CRT alone, the ICER for nodal staging surgery was $19,505/QALY (Table 3).
2. Sensitivity analysis
One-way sensitivity analyses were performed on selected variables in the model across the ranges specified in Table 4. In the base-case model, a 30% reduction in survival is assumed if patients undergo pelvic CRT despite the presence of occult PALN metastasis. As the true effect of unstaged PALN metastasis is unknown in LACC, the percentage reduction in survival was varied for sensitivity analysis. The model was relatively sensitive to changes in survival reduction in patients who undergo pelvic CRT despite the presence of occult PALN metastasis (cohort 2) compared to those who had nodal staging surgery followed by tailored CRT as a result of PALN metastasis (cohort 3). When the reduction in survival was less than 17%, the ICER per QALY saved increases to $50,000, and when the reduction in survival was less than 12%, the ICER increased to $100,000 per QALY saved. The model was insensitive to changes in the performance of PET/CT and postoperative complication rates when rates were varied over clinically reasonable ranges. Nodal staging surgery followed by tailored CRT was more cost-effective than pelvic CRT alone, as the ICER did not exceed $50,000/QALY so long as the false-negative rate for PET/CT is higher than 5%. If postoperative complication rates were below 30%, ICER did not exceed $60,000/QALY.
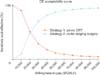
A probabilistic sensitivity analysis was conducted using a Monte Carlo simulation of 10,000 trials. The acceptability curve, depicted in Fig. 2, shows a comparison between the two strategies. Probabilistic sensitivity analysis demonstrates the robustness of the base-case results, with a 48%, 82%, and 91% probability of cost-effectiveness at the willingness-to-pay thresholds of $20,000/QALY, $40,000/QALY, and $60,000/QALY, respectively.
DISCUSSION
To date, there is no absolute threshold of cost-effectiveness that policy-makers will consider for a strategy to be acceptable. In the US, $50,000 per QALY is frequently cited as being cost-effective. The ICER threshold in South Korea has not been determined officially. The 'World Health Report 2002' suggests that an intervention that costs less than three times the gross domestic product (GDP) per capita for each disability-adjusted life year is cost-effective. As GDP per capita in South Korea in 2011 was $21,539, a willingness-to-pay threshold of $60,000/QALY (around three times the Korean GDP per capita) is used to define a cost-effective strategy from the standpoint of resource utilization in the Korean healthcare system [2324].
In this study, a cost-effectiveness analysis was performed that compared two strategies LACC; the results showed that nodal staging surgery followed by tailored CRT is a cost-effective treatment option within clinically acceptable range of variables. To date, no studies have evaluated the cost-effectiveness of nodal staging surgery in the era of PET/CT.
A major limitation of our study is the lack of survival data for unstaged PALN metastasis in the model as no prospective trial has been performed that compares the outcomes of nodal staging followed by tailored CRT and pelvic CRT without surgical staging in the era of PET/CT. The base-case scenario assumes a 30% reduction in overall survival when patients undergo pelvic CRT despite the presence of occult PALN metastasis. Our model is clearly sensitive to changes in survival differences between patients who undergo pelvic CRT and those with who have nodal staging surgery in cases with occult PALN metastasis. Nodal staging surgery followed by tailored CRT is cost-effective (ICER <$60,000) when survival reduction falls within a clinically reasonable range. At the baseline false-negative rate for PET/CT detecting PALN metastasis (12%), a 15% reduction in the survival rate for patients with unstaged PALN metastasis indicates that the 5-year overall survival rate for strategy 2 is higher than for strategy 1 by approximately 1.7%. Although no randomized trials evaluate the role of surgical staging in the era of PET/CT, prospective studies suggest that nodal staging surgery followed by extended-field CRT provides survival gains for patients with PALN metastases measuring 5 mm or less metastases that would probably be missed by PET/CT [1225].
Other one-way sensitivity analyses show the robustness of our cost-effectiveness results. The proportion of cases of PALN metastasis showing no uptake on PET or PET/CT but proven by histologic analysis to be positive (false-negative rate) was 5% to 17%. Nodal staging surgery followed by tailored CRT is cost-effective for a wide range of false-negative rates for PET/CT detecting PALN metastasis. Moreover, morbidity following surgical staging should be considered together with possible perioperative and late adverse effects. Although we consider only lymphocele and lymphedema, an extraperitoneal approach is shown to reduce perioperative morbidity and particularly the incidence of RT-induced complications [26]. The incidence rates for lymphocele and lymphedema that require intervention following nodal staging surgery are within tolerable range (less than 10%) when performed by highly skilled surgeons [25]. Our model shows that nodal staging surgery is cost-effective with a wide range of postoperative complication rates.
If PET/CT shows negative findings for PALN metastasis, we assume that any occult PALN metastases (unstaged PALN) measure less than 5 mm at the time of surgical staging. Some showed that the survival rate for patients with PALN metastases measuring 5 mm or less (when treated with nodal staging surgery followed by extended-field CRT) is similar to that of women without PALN metastasis [12]. However, a considerable proportion of cases where PALN metastases measure more than 5 mm (6.8%) was found in a prospective trial despite negative uptake in PET/CT [25]. Gouy et al. [25] demonstrated that the event-free survival rate at 3 years in patients with PALN metastases measuring more than 5 mm was just 17%. For PALN involvement greater than 5 mm in particular, the survival gains from nodal staging surgery followed by extended-field CRT are not clear. Therefore, the survival outcome of nodal staging surgery followed by tailored CRT reported in this study may be overestimated.
Other limitations of this study include the assumption that there was no delay in the administration of definite CRT after nodal staging surgery. A major drawback of nodal staging surgery is the resultant delay in starting curative treatment, attributable to either an overburdened surgical schedule or postoperative morbidity [27].
Despite these limitations, our model provides an insight into how clinicians might approach treatment decisions for patients with LACC. Based on previous results, a considerable proportion of patients have PALN metastasis even when no uptake is found in PET/CT. Nodal staging surgery followed by extended-field CRT can be expected to improve survival outcomes in this subgroup without adding a significant economic burden.
In conclusion, nodal staging surgery before CRT is potentially cost-effective in clinically acceptable ranges for LACC when PET/CT shows no evidence of PALN metastasis. While definite data are needed to confirm our results, this study demonstrates the merit of incorporating nodal staging surgery in future prospective trials. This study opens up discussion of the possibility that nodal staging surgery may be cost-effective in the era of PET/CT. Prospective trials are warranted to transfer these results to guidelines.





 XML Download
XML Download