

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The nodal station No. 14v (along the superior mesenteric vein) was previously included in the D2 dissection criteria, but is no longer recommended by the Japanese Gastric Cancer Treatment Guidelines [1]. However, this nodal station is still defined as part of the regional gastric lymph nodes, and the role of a No. 14v lymphadenectomy is still controversial. In the 2014 Japanese Gastric Cancer Treatment Guidelines (version 4), the potential benefits of a No. 14v dissection for patients with No. 6 nodal metastases were only suggested, not prescribed, because scientific evidence is lacking [2]. Many surgeons believe that there is lymphatic flow from nodal station No. 6 to No. 14v. This lymphatic flow is important because No. 14v is a pivotal gateway to a possible systemic spread of cancer.
In the present case, a patient initially underwent laparoscopic distal gastrectomy with D1+ dissection for early gastric cancer; metastases in the No. 6 lymph nodes were recognized pathologically post-surgery (pT1bN1M0, p-Stage 1B). The patient then had recurrence at the No. 14v nodal station 4 months after the initial surgery. A second surgery excising the recurrent tumor at the No. 14 nodal station was then carried out, and the patient has achieved long-term survival without recurrence.
CASE REPORT
A 73-year-old woman presented at the hospital with heart burn symptoms. Upper gastrointestinal endoscopy showed a type 0–I tumor at the greater curvature of the antrum (Fig. 1). Pathological diagnosis of the biopsy specimen was determined as differentiated adenocarcinoma. Based on examination, the patient was diagnosed with T1aN0M0, c-Stage IA gastric cancer, and an endoscopic submucosal dissection (ESD) was subsequently performed. The operation time was 75 minutes, and an en bloc resection without perforation was achieved (Fig. 2). The pathological diagnosis of the ESD specimen was adenocarcinoma (tub1>tub2, pT1b (invades up to 1/3 of submucosa [sm1]; 450 µm), INFb, int, ly3, v0, pHM0, pVM0, pType 0–IIa+IIc, 40×29 mm), which requires non-curative resection according to the criteria defined in the Japanese Gastric Cancer Treatment Guidelines [2]. The patient opted for additional surgery. Preoperative computed tomography (CT) did not reveal either swollen lymph nodes or metastatic lesions. The patient underwent laparoscopic distal gastrectomy with D1+ lymph node dissection. During the operation, there was no evidence of lymph node metastases in the infra-pyloric area; thus, an intra-operative frozen section procedure was not performed. However, pathological examination of the permanent section revealed 2 nodal metastases at the No. 6 nodal station. Therefore, the patient was diagnosed with pT1bN1M0, p-Stage IB (lymph nodes 2/28) gastric cancer. There was no postoperative complication and she was discharged from the hospital 8 days post-surgery.
Fig. 1
Endoscopic view of the lesion before ESD. Upper gastrointestinal endoscopy revealed an elevated tumor (Type 0–I) at the greater curvature of the antrum.
ESD = endoscopic submucosal dissection.
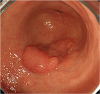
Fig. 2
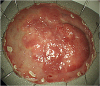
Specimen from endoscopic submucosal resection. En bloc resection was achieved without perforation.
Four months after radical surgery, a follow-up CT revealed an enlarged nodule (14×12 mm) at the left side of the superior mesenteric vein (Fig. 3). Positron emission tomography (PET)-CT imaging was also performed, which demonstrated mild fluorodeoxyglucose uptake at the same site with a standardized uptake value of 3.8 (Fig. 4). No other lesion indicating distant metastasis was observed. Levels of tumor markers, carcinoembryonic antigen, and carbohydrate antigen 19-9 were within normal ranges. Thus, recurrence was suspected at nodal station No. 14v. Excision of the lesion with lymph node dissection of No. 14v and 14a areas was performed. The operation was executed with a mini-laparotomy with a total operation time of 54 minutes, and a small quantity of blood loss. No postoperative complication was observed, and the patient was discharged 6 days post-surgery. Pathological findings revealed that the enlarged nodule was metastatic adenocarcinoma. There were no signs of malignancy in the other 2 harvested lymph nodes. Adjuvant chemotherapy of tegafur-gimeracil-oteracil potassium (S-1) (80 mg/m2) was given for 1 year. The patient has a current survival of 5.5 years after the second operation without recurrence.
Fig. 3
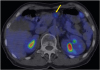
CT image showing a nodule 14×12 mm in size (yellow arrow), detected at the left side of the superior mesenteric vein.
CT = computed tomography.

DISCUSSION
Initially, there was ambiguity regarding the correct numbering of the recurrence site, and to which nodal station it was categorized, either No. 14v or 14a. The epicenter of the nodule appeared to be in front of the superior mesenteric artery, but was exceeding the line of the left rim of the superior mesenteric vein. This led to the determination that it should be numbered as No. 14v. In clinical terms, strict distinction between No. 14v and 14a is not crucial.
The incidence of lymphatic recurrence after radical surgery for early gastric cancer is reported to be 7%–8% [34]. Furthermore, the most dominant sites of recurrence are hematogenous followed by lymphatics [45]. The median interval from surgery to recurrence is 26 months (range, 3–98), with recurrence occurring within 5 years of surgery in most cases [4]. In the present case, the interval between surgery and recurrence was only 4 months. Therefore, it is speculated that undetected metastasis at the No. 14v nodal station was present at the time of initial surgery, which then grew rapidly due to immunosuppression caused by surgical stress.
The significance of No. 14v lymph node dissection for advanced gastric cancer is still debatable. A retrospective study have reported an impact on survival from D2+ No. 14v dissection, especially in c-Stage III or IV gastric cancer of the middle or lower gastric body [6]. In contrast, some researchers have reported that the No. 14v lymph node metastasis is a poor prognostic factor, and can be regarded as distant metastasis [7]. Meanwhile, the rate of No. 14v lymph node metastases in T1a and T1b early gastric cancer is reported to be lower: 0.0% and 0.7%, respectively [8]. Additionally, some studies have emphasized that a No. 6 metastasis is a pivotal risk factor for a No. 14v metastasis [9]. In addition to the presented case, previous studies demonstrate that there is a lymphatic pathway from the infra-pyloric area to around the mesenteric superior vein/artery. If a No. 6 metastasis had been observed during the initial surgery in the present case, a No. 14v dissection would have been executed. One drawback of laparoscopic surgery is the loss of tactile sense. Lymph node status of the resected specimen is carefully checked on a back table when performing laparoscopic surgery at our institution. However, an intra-operative frozen section procedure is always crucial when a No. 6 metastasis is suspected during surgery. If this frozen section is proved to be a metastasis, the No. 14v nodal station is dissected, even in early-stage disease.
Necessity of a No. 12a and No. 11p nodal dissection at the second operation are possible discussion points because they are included in the extent of D2 dissection in distal gastrectomy. However, this was not performed for the following reasons: no obvious swollen nodes at these areas in the CT scan before the second operation; the absence of metastases to other suprapancreatic or lesser curvature's nodal stations at the initial operation; and expected technical difficulties, as well as risks associated with postoperative adhesions around the suprapancreatic area.
Another crucial point in the current study is that long-term survival was achieved after excision of the metastatic lesion combined with subsequent adjuvant chemotherapy. This suggests that metastasis at the No. 14v nodal station does not always means systemic metastasis or the extensive spread of cancer cells. In recurrent cases, chemotherapy (S-1 plus cisplatin) is the first choice of therapy according to the latest guidelines [210]. However, when recurrence was detected for the present case, surgery was selected instead of systemic chemotherapy for the following reasons. First, there was no indication that the nodule was metastatic because the duration from surgery was too short. Second, since the location of the lesion was solitary and accessible from the abdominal wall, the second operation appeared simple. If the recurrence site had been at the No. 16 nodal station, systemic chemotherapy would have been first selected.
Currently, we have minimal evidence to discuss the role of a No. 14v nodal station dissection for gastric cancer, and a comprehensive analysis is necessary. However, when a No. 6 metastasis is recognized, the possibility of a concurrent No. 14v metastasis should be considered, even in early gastric cancer. Even in cases where there is a No. 14v metastasis, some patients can achieve long-term survival.
 XML Download
XML Download