

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
While the safety and efficacy of laparoscopic adrenalectomy are relatively well documented, this procedure remains challenging for pheochromocytoma. The purpose of our investigation was to assess the perioperative profiles of laparoscopic adrenalectomy (LA) with those of open adrenalectomy (OA) in patients with pheochromocytoma.
Materials and Methods
Between January 1997 and October 2005, 31 patients with pheochromocytoma underwent surgical removal, including 15 LA and 16 OA. The LA was performed via a lateral decubitus transperitoneal approach. The mean tumor size was similar in both groups (LA 6.0cm vs. OA 5.7cm). All patients underwent extensive preoperative medical preparation with alpha-blockers. The intraoperative hemodynamic instabilities and perioperative profiles were retrospectively analyzed.
Results
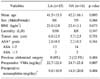
No conversion to open surgery was required with either procedure and no mortality was observed. Hypertensive crisis (systolic blood pressure>200mmHg) and severe tachycardia (heart rate>100/min) were more common in the OA group (LA 13.3 and 26.7% vs. OA 56.3 and 62.5%). The mean operating times for both groups were similar (LA 182.0±47.0 min vs. OA 183.1±66.5 min), but the duration of hospitalization was shorter in the LA group (LA 5.3±2.2 days vs. OA 6.8±1.0 days). The estimated blood loss was greater in the OA group (LA 103.3±44.2ml vs. OA 159.4±66.8ml). Intravenous morphine was needed in 56.3% of the OA, but in only 13.3% of the LA group. There were no significant differences in the postoperative complications between the two groups.



References
1. Gagner M, Lacroix A, Bolte E. Laparoscopic adrenalectomy in Cushing's syndrome and pheochromocytoma. N Engl J Med. 1992. 327:1033.
2. Lee AK, Park KJ, Kim HH, Choi H. Experience of transperitoneal laparoscopic adrenalectomy: initial 4 cases. Korean J Urol. 2000. 41:408–413.
3. Kim MK, Yu HC, Kim HJ. Transperitoneal laparoscopic versus open adrenalectomy: a comparative study. Korean J Urol. 2001. 42:1295–1298.
4. Kim TN, Lee JZ, Chung MK, Kim IJ, Kim YK, Lee W. Clinical experience of laparoscopic adrenalectomy. Korean J Urol. 2005. 46:931–937.
5. Assalia A, Gagner M. Laparoscopic adrenalectomy. Br J Surg. 2004. 91:1259–1274.
6. Naya Y, Ichikawa T, Suzuki H, Komiya A, Nagata M, Ueda T, et al. Efficacy and safety of laparoscopic surgery for pheochromocytoma. Int J Urol. 2005. 12:128–133.
7. Del Pizzo JJ, Schiff JD, Vaughan ED. Laparoscopic adrenalectomy for pheochromocytoma. Curr Urol Rep. 2005. 6:78–85.
8. Guerrieri M, Baldarelli M, Scarpelli M, Santini S, Lezoche G, Lezoche E. Laparoscopic adrenalectomy in pheochromocytomas. J Endocrinol Invest. 2005. 28:523–527.
9. Kazaryan AM, Kuznetsov NS, Shulutko AM, Beltsevich DG, Edwin B. Evaluation of endoscopic and traditional open approaches to pheochromocytoma. Surg Endosc. 2004. 18:937–941.
10. Edwin B, Kazaryan AM, Mala T, Pfeffer PF, Tonnessen TI, Fosse E. Laparoscopic and open surgery for pheochromocytoma. BMC Surg. 2001. 1:2.
11. Welbourn RB. Early surgical history of phaeochromocytoma. Br J Surg. 1987. 74:594–596.
12. Niemann U, Hiller W, Behrend M. 25 years experience of the surgical treatment of phaeochromocytoma. Eur J Surg. 2002. 168:716–719.
13. Werbel SS, Ober KP. Pheochromocytoma. Update on diagnosis, localization, and management. Med Clin North Am. 1995. 79:131–153.
14. Marty J, Desmonts JM, Chalaux G, Fischler M, Michon F, Mazze RI, et al. Hypertensive responses during operation for phaeochromocytoma: a study of plasma catecholamine and haemodynamic changes. Eur J Anaesthesiol. 1985. 2:257–264.
15. Newell KA, Prinz RA, Brooks MH, Glisson SN, Barbato AL, Freeark RJ. Plasma catecholamine changes during excision of pheochromocytoma. Surgery. 1988. 104:1064–1073.
16. Joris JL, Hamoir EE, Hartstein GM, Meurisse MR, Hubert BM, Charlier CJ, et al. Hemodynamic changes and catecholamine release during laparoscopic adrenalectomy for pheochromocytoma. Anesth Analg. 1999. 88:16–21.
17. Rocha MF, Tauzin-Fin P, Vasconcelos PL, Ballanger P. Assessment of serum catecholamine concentrations in patients with pheochromocytoma undergoing videolaparoscopic adrenalectomy. Int Braz J Urol. 2005. 31:299–307.
18. Mobius E, Nies C, Rothmund M. Surgical treatment of pheochromocytomas: laparoscopic or conventional? Surg Endosc. 1999. 13:35–39.
19. Sprung J, O'Hara JF Jr, Gill IS, Abdelmalak B, Sarnaik A, Bravo EL. Anesthetic aspects of laparoscopic and open adrenalectomy for pheochromocytoma. Urology. 2000. 55:339–343.
20. Gagner M, Breton G, Pharand D, Pomp A. Is laparoscopic adrenalectomy indicated for pheochromocytomas? Surgery. 1996. 120:1076–1079.
21. Fernandez-Cruz L, Saenz A, Taura P, Sabater L, Astudillo E, Fontanals J. Helium and carbon dioxide pneumoperitoneum in patients with pheochromocytoma undergoing laparoscopic adrenalectomy. World J Surg. 1998. 22:1250–1255.
22. Gonzalez R, Smith CD, McClusky DA 3rd, Ramaswamy A, Branum GD, Hunter JG, et al. Laparoscopic approach reduces likelihood of perioperative complications in patients undergoing adrenalectomy. Am Surg. 2004. 70:668–674.
23. Gagner M, Pomp A, Heniford BT, Pharand D, Lacroix A. Laparoscopic adrenalectomy: lessons learned from 100 consecutive procedures. Ann Surg. 1997. 226:238–246.
24. Kercher KW, Novitsky YW, Park A, Matthews BD, Litwin DE, Heniford BT. Laparoscopic curative resection of pheochromocytomas. Ann Surg. 2005. 241:919–926.
25. Jaroszewski DE, Tessier DJ, Schlinkert RT, Grant CS, Thompson GB, van Heerden JA, et al. Laparoscopic adrenalectomy for pheochromocytoma. Mayo Clin Proc. 2003. 78:1501–1504.
26. Kim AW, Quiros RM, Maxhimer JB, El-Ganzouri AR, Prinz RA. Outcome of laparoscopic adrenalectomy for pheochromocytomas vs aldosteronomas. Arch Surg. 2004. 139:526–529.
27. Gill IS. The case for laparoscopic adrenalectomy. J Urol. 2001. 166:429–436.
 XML Download
XML Download