

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
According to the presence of proper muscle in the resected specimens from primary T1G3 bladder tumors, we compared the prognosis and investigated factors that were predictive of disease progression during the follow-up and upstaging after radical cystectomy.
Materials and Methods
We reviewed the records of 157 patients who were diagnosed with primary T1G3 bladder cancer for the assessment and comparison of disease recurrence, disease progression and patient survival. There were 101 and 56 patients with and without proper muscle in the their transurethral resection (TUR) specimens (T1G3 and T1xG3, respectively); 30 and 20 of these patients, respectively, had undergone immediate cystectomy.
Results
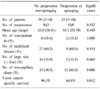
Among the patients who were followed up after transurethral surgery, there were no differences in the survival between the two groups. For the patients treated by immediate cystectomy, the 5-year cancer-specific survival was 100% for the T1G3 patients at a mean follow-up of 54.5 months while it was 76.6% for the T1xG3 patients at a mean follow-up of 46.0 months (p=0.042). With the absence of radiologic findings suggestive of invasive bladder cancer, 55.6% of the T1xG3 patients were upstaged after radical cystectomy, whereas only 12.0% of the T1G3 patients were upstaged (p=0.002). Between the followed-up group and the cystectomy groups, more patients in the cystectomy group had non-papillary shaped bladder tumor (75.0% vs. 38.9%, respectively, p=0.010). Similarly, the T1x-G3 patients who progressed during follow-up or who were upstaged after radical cystectomy had more non-papillary shaped tumor than the patients who were without progression or upstaging (80.1% vs. 38.5%, respectively, p=0.006).
Figures and Tables
Fig. 1
The cancer-specific survival according to the presence of proper muscle in the transurethral resection (TUR) specimen. T1G3: T1G3 bladder cancer with proper muscle in the TUR specimen; T1xG3: T1G3 bladder cancer without proper muscle in the TUR specimen. (A) Follow-up groups, (B) immediate cystectomy groups.

Table 2
Upstaging after radical cystectomy according to the presence of suspicious radiology* and proper muscle in transurethral resection (TUR) specimen


References
1. Jakse G, Loidl W, Seeber G, Hofstadter F. Stage T1, grade 3 transitional cell carcinoma of the bladder: an unfavorable tumor? J Urol. 1987. 137:39–43.
2. Cookson MS, Sarosdy MF. Management of stage T1 superficial bladder cancer with intravesical bacillus Calmette-Guerin therapy. J Urol. 1992. 148:797–801.
3. Pansadoro V, Emiliozzi P, de Paula F, Scarpone P, Pansadoro A, Sternberg CN. Long-term follow-up of G3T1 transitional cell carcinoma of the bladder treated with intravesical bacille Calmette-Guerin: 18-year experience. Urology. 2002. 59:227–231.
4. Baniel J, Grauss D, Engelstein D, Sella A. Intravesical bacillus Calmette-Guerin treatment for stage T1 grade 3 transitional cell carcinoma of the bladder. Urology. 1998. 52:785–789.
5. Thalmann GN, Markwalder R, Shahin O, Burkhard FC, Hochreiter WW, Studer UE. Primary T1G3 bladder cancer: organ preserving approach or immediate cystectomy? J Urol. 2004. 172:70–75.
6. Herr HW. Tumour progression and survival in patients with T1G3 bladder tumours: 15-year outcome. Br J Urol. 1997. 80:762–765.
7. Dutta SC, Smith JA Jr, Shappell SB, Coffey CS, Chang SS, Cookson MS. Clinical under staging of high risk nonmuscle invasive urothelial carcinoma treated with radical cystectomy. J Urol. 2001. 166:490–493.
8. Grimm MO, Steinhoff C, Simon X, Spiegelhalder P, Ackermann R, Vogeli TA. Effect of routine repeat transurethral resection for superficial bladder cancer: a long-term observational study. J Urol. 2003. 170:433–437.
9. Stockle M, Alken P, Engelmann U, Jacobi GH, Riedmiller H, Hohenfellner R. Radical cystectomy--often too late? Eur Urol. 1987. 13:361–367.
10. Smith JA Jr, Labasky RF, Cockett AT, Fracchia JA, Montie JE, Rowland RG. The American Urological Association. Bladder cancer clinical guidelines panel summary report on the management of nonmuscle invasive bladder cancer (stages Ta, T1, and TIS). J Urol. 1999. 162:1697–1701.
11. Herr HW, Donat SM, Dalbagni G. Correlation of cystoscopy with histology of recurrent papillary tumors of the bladder. J Urol. 2002. 168:978–980.
12. McDonald JR, Thompson GJ. Carcinoma of the urinary bladder: a pathologic study with special reference to invasiveness and vascular invaion. J Urol. 1948. 61:435–439.
13. Cha KB, Chung BH, Hong SJ. Clinical manifestation of tumor-recurrence and progression after transurethral resection and BCG intravesical instillation in patients with T1G3 bladder cancer. Korean J Urol. 2002. 43:490–495.
14. Schrier BP, Hollander MP, van Rhijn BW, Kiemeney LA, Witjes JA. Prognosis of muscle-invasive bladder cancer: difference between primary and progressive tumours and implications for therapy. Eur Urol. 2004. 45:292–296.
 XML Download
XML Download