

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Endometriosis is defined as the presence of endometrial glands and stroma at extra-uterine sites. These ectopic endometrial implants are usually located on the ovaries. But it can be observed on the uterus and its ligaments, in the abdominal cavity, on the cervix, pleura, and very rarely in the lungs, brain, and eyes. Namely, it can occur nearly anywhere in the body.
Many patients with cervix endometriosis are asymptomatic. By reviewing literature, we can find a diverse range of persistent symptoms which is abnormal pap smear, post-coital bleeding, pelvic pain, intermenstrual bleeding and massive hemorrhage.1~5 Cervix endometriosis may be a source of glandular cells in cervical smears and hence a cause of abnormal smear result. So it can lead to misjudge as cervix cancer. A considerable number of patients reported in the literature only had abnormal smear results and were diagnosed during colposcopy or by histopathological examinations of their biopsy or hysterectomy specimens. But, adenocarcinoma arising from cervix endometriosis has been reported in literature.6,7 This provides the reason to interested in the disease in detail.
In 1928 cervical endometriosis was first mentioned by Fels. After that, many case reports had been accumulated in literature. However there is paucity of knowledge in literature regarding cervix endometriosis. Limited awareness of the clinical appearance of the disease may account for its apparent rarity.
We recently encountered a case of cervical endometriosis in post-menopause woman. To remind clinician of the neglected issue of endometriosis of the cervix, we report a case of cervical endometriosis with literature review.
Case Report
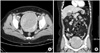
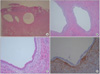
54-year-old woman was referred to Soonchunhyang University Hospital with the suspicion of huge myoma uteri from local clinics. Having had two full term vaginal deliveries, she has been menopause state three years ago without hormone therapy. Routine pap smear showed reactive cellular changes with inflammation and human papillomavirus (HPV) deoxyribonucleic acid (DNA) Chip test was negative. Ultrasound examination and computed tomography (CT) revealed 11.0 × 9.0 × 10.2 cm sized mass in uterine fundus and body portion (Fig. 1). On physical examination, the patient was generally well, weighed 74.9 kg and not pale. General examination was unremarkable. Hematological examination was within normal range. The patient underwent laparoscopy assisted vaginal hysterectomy on June 14, 2011. At operation, there was no evidence of endometriosis. Grossly the uterus was diffusely enlarged, weighed 735 gm. Microscopically, both endometrial glands and stroma present at the cervical stroma (Fig. 2). Pathologic findings indicate that there was endometriosis at cervix, atrophy at endometrium, and leiomyoma at myometrium.
Discussion
English-language published literatures from 1970 to 2011 were searched on the PubMed database using the keywords 'cervix endometriosis'. A total of 45 papers related to cervix endometriosis were retrieved from the database. From these papers, the incidence of cervix endometriosis has been reported to be between 1.6% to 2.4%.8 Endometriosis was estrogen dependent disease. So cervix endometriosis in post-menopause women has been much rarely occurred. Even though the post-menopause endometriosis is rarely associated with cancer, gynecologists should pay attention to management for this disease. Kim et al. have presented two case of endometriosis detected in post-menopause women and a case of serous adenocarcinoma arising from ovarian endometriosis after menopause.9,10
There is no symptoms in all women with cervix endometriosis. Abnormal pap smear result is a common presentation. Baker et al. described a series of 20 cases of superficial endometriosis of the cervix in 1999.11 The majority of the patients were referred because of abnormal uterine cervical lesions like endocervical glandular dysplasia, adenocarcinoma in situ (ACIS) or, rarely, an invasive carcinoma of the cervix. And cervix endometriosis was incidentally discovered. Cervix endometriosis might be the cause of abnormal smears, because the cytomorphological features of endometriosis cells change with the cyclical hormonal changes, and sometimes revealed crowded, overlapping glandular cells with loss of cell polarity and rosette formations. These cytological features would be sufficient to overlap with precancerous and cancerous glandular lesions. Therefore if one is unaware of the presence of cervix endometriosis, the condition can be diagnosed as 'atypical glandular cells'.12
Several theories have been proposed to explain pathogenesis of cervix endometriosis. Many investigators commonly account for the pathogenesis of cervix endometriosis as implantation of cast-off endometrial fragments on the previously traumatized lesion of cervix. Cervix endometriosis is generally considered as rare lesion. But with widespread use of invasive cervical procedure an increased incidence of cervical endometriosis can be expected. However, as in our case, cervix endometriosis can be encountered in patients who never underwent procedures traumatizing the cervix. This might be explained by Hoang et al hypothesised that cervix endometriosis could develop in mullerian rests which persist in the stroma of the cervix.13
In summary, not uncommonly, cervix endometriosis is diagnosed after operation. The clinical feature is very diverse. In our case, the woman was post-menopause state without hormone therapy. There was only reactive cellular change in her pap smear result. She never underwent traumatic procedure of cervix. Like this case, to most post-menopause women, cervix endometriosis would be the only incidental finding. But cervix endometriosis in post-menopause women was rare and interesting finding. Many post-menopause women would undergo operation because of other pathology and after operation cervix endometriosis could be incidentally diagnosed by histopathology. With increased use of hormone therapy, cervix endometriosis in post-menopause could be shown different clinical features. We thought that studying cervix endometriosis in post-menopause women with or without hormone therapy would be interesting.
 XML Download
XML Download