

 PDF
PDF ePub
ePub Citation
Citation Print
Print


The purpose of the present study was to investigate the causes of impingement between the patella bone and the bearing post during high flexion in the cruciate-substituting total knee arthroplasty and propose a treatment strategy. Cruciate ligament-substituting total knee arthroplasty has the advantage of greater flexion of the knee joint and enables normal knee dynamic motion by allowing the femoral roll back phenomenon while bending.12345) However, patella impingement, patellotibial impingement, and fat pad impingement following total knee arthroplasty are the known causes of anterior knee pain; and the methods for preventing anterior knee pain include change in bearing design and intraoperative removal of the fat pad.678910) In some patients with an expected knee joint movement of more than 130° in the operative field, the range of motion is less than 110° due to anterior knee pain caused by impingement between the patella bone and the bearing post after mobile and fixed type total knee arthroplasty; these patients were treated by resection of the lower articular part of the patella bone and the impinged soft tissue. Therefore, impingement between the patella bone and the bearing post after total knee arthroplasty was one of the causes of less than 120° knee flexion. Since Koreans prefer kneeling and squatting postures for various cultural purposes even after total knee arthroplasty, 130° or higher knee flexion is required. Hence, we conducted this prospective cohort study to determine the causes of impingement and methods to prevent impingement between the patella bone and the bearing post after total knee arthroplasty.
METHODS
This prospective cohort study included 218 cases that underwent cruciate ligament-substituting total knee arthroplasty from February 2014 to January 2015; a single surgeon performed the operation using the same method without patellar resurfacing in all patients. The lateral patellofemoral ligament and the retinaculum were released, and extensive osteophytes were removed from the patella bone. During surgery, a goniometer was used after insertion of a trial bearing to determine the angle at which impingement occurs between the bearing post and the patella bone when the knee was moved from 90° flexion to full flexion. In this study, impingement was considered positive when contact between the patella bone and the bearing post occurred at knee flexion of 120° or forward displacement of the patella occurred owing to impingement. The study included 139 female and 13 male patients with an average age of 70.6 years (range, 54 to 89 years).
The patients were divided into the Biomet mobile type-bearing group (rotating platform knee) and the Corentec fixed-type bearing group (Lospa; Corentec, Seoul, Korea) to compare the impingement frequency; statistical significance was according to implant design.
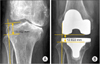
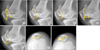
Changes to the joint line were measured at pre- and postoperative standing knee anteroposterior (AP) radiographic views. The most proximal point of the fibula head was selected as the reference point for this study because fibula head enables easy viewing, and is used by many authors. 111213) Measurements were taken by one author (SS), and the methods used were as follows: the preoperative joint line was defined as a line through the midpoint of the lateral knee joint gap that is the perpendicular line to the long axis of the fibula, and the postoperative joint line was defined as a line that contacts the lowest point of the lateral femoral component that is the perpendicular line to the long axis of the fibula. In addition, to determine the height of the joint line, we measured the distance from the top of the fibular head to the levels of preoperative and postoperative joint lines (Fig. 1). Moreover, images in the 30-degree flexion lateral view and Merchant view were obtained for pre- to postoperative changes in the location of the patella bone (Insall-Salvati ratio) and the anatomical configurations of the patella bone; while the preoperative angle and the length of patella bone were measured with the osteophytes included (Fig. 2). Patella bone location, anatomical configurations of the patella bone, and size of the inserted implants was compared in the fixed-type bearing group alone, in order to investigate the statistical significance between the cause of impingement occurrence with changes in joint line.
In addition, interrelationships between the size of the inserted implants and occurrence of impingement were assessed. Chi-square test was performed in the fixed-type bearing group (124 cases) to determine the increased risk of impingement with a smaller size femoral implant.
Univariate analysis, matching sample t-test, and chi-square test were used for clinical and radiological evaluations. SPSS ver. 12.0 (SPSS Inc., Chicago, IL, USA) was used to determine the statistical significance when the p-value was < 0.05.
RESULTS
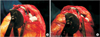
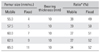
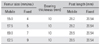
Demographics were shown in Table 1. Among the mobile-type Biomet bearing cases, impingement occurred in 90 of the 94 cases; and among the fixed-type Corentec bearing cases (n = 124), impingement occurred only in 47 of the 124 cases; impingement incidence was more common in patients with mobile bearing that was relatively more anteriorly located and those with a longer post than in those with a fixed bearing (Tables 2 and 3, Fig. 3). There was a statistically significant correlation between impingement and the type of implants (p = 0.04).
The average height of the joint line in the fixed-type bearing group (n = 124) was 14.0 mm before surgery and 13.1 mm after surgery. The joint line height decreased from 13.5 mm to 12.6 mm in the impinged cases (n = 47), and from 14.2 mm to 13.4 mm in the cases without impingement (n = 77). There was no statistically significant correlation between impingement and changes in the joint line (p = 0.069).
Changes in the patella bone location (Insall-Salvati ratio) was from 1.15 before surgery to 1.09 after the surgery in the fixed-type bearing group (n = 124). The reduction in Insall-Salvati ratio was from 1.14 to 1.08 in cases with impingement (n = 47), and from 1.15 to 1.10 in cases without impingement (n = 77). There was no significant correlation between impingement and changes in patellar bone location between groups (p = 0.51).
The probability of impingement occurrence according to the characteristics of patellar shape in patients with fixed-type bearing (n = 124), was determined by measuring the patella length-articular ratio, the patella nonarticular-articular ratio, the patella articular-nonarticular angle, the patella length, the patella inner thickness ratio, the patella inferior pole angle, the patella facet angle, and the patella inner thickness ratio.
The patella length-articular average ratio was 0.68 in the impingement cases (n = 47) and 0.70 in cases without impingement (n = 77); without significant correlation between the 2 groups (p = 0.575) (Fig. 2A). The patella nonarticular-articular average ratio was 2.32 in cases with impingement (n = 47) and 2.40 in cases without impingement (n = 77); without significant correlation between the 2 groups (p = 0.69) (Fig. 2B). However, the average length of the posterior articular surface from 32.4 mm to 27.0 mm to 5.4 mm following excision of the patella bone because of impingement. The patella articular-nonarticular average angle was 129.2° in cases with impingement (n = 47), and 129.4° in cases without impingement (n = 77); without significant correlation between the 2 groups (p = 0.384) (Fig. 2C). The average patella length was 44.9 mm in cases with impingement (n = 47), and 40.3 mm in cases without impingement (n = 77); with a statistically significant correlation between the 2 groups (p = 0.04) (Fig. 2D). The patella bone inner thickness average ratio under lateral view was 0.20 in the cases with impingement (n = 47), and 0.23 in the cases without impingement (n = 77); without significant correlation between the 2 groups (p = 0.148) (Fig. 2D). In addition, the average thickness of the articular side of the patella lateral view was 9.1 mm in the cases with impingement (n = 47), and 9.1 mm in the cases without impingement (n = 77); without significant correlation between the 2 groups (p = 0.25) (Fig. 2D). The patella inferior pole average angle was 37.7° in cases with impingement (n = 47), and 30.5° in cases without impingement (n = 77); without significant correlation between the 2 groups (p = 0.03) (Fig. 2E). The patella bone facet average angle was 117.1° in cases with impingement (n = 47), and 119.6° in cases without impingement (n = 77); without significant correlation between the 2 groups (p = 0.414) (Fig. 2F). The patella bone inner thickness average ratio under the Merchant view was 0.25 in cases with impingement (n = 47), and 0.25 in cases without impingement (n = 77); without significant correlation between the 2 groups (p = 0.301) (Fig. 2G).
In the fixed-type bearing group (124 cases), impingement occurrence showed significant correlation with smaller size femoral implant (p = 0.01). However, according to manufacturer-recommended compatibility between the femoral and tibial implants, impingement occurred in 33 of the 88 cases in which the implant size coincided, and in 13 of the 36 cases in which the implant size did not coincide; without significant correlation (p = 0.684).
The impingement between the patella bone and the bearing post causes forward displacement of the patella bone; furthermore, the forward displacement of the patella increases as knee flexion increases after impingement. Forward displacement of the patella can lead to stretching of the patellofemoral ligament and retinaculum and a reduction in the flexion gap. Therefore, the cases with impingement were treated by resection of the lower portion of the patella, without resultant forward displacement of the patella (Figs. 4 and 5).
DISCUSSION
We hypothesized that the design or size of the implant, changes in the height of the joint line prior to and after the surgery, shape of the patella bone, changes in the height of the patella bone, and discordance in the sizes of the femoral and tibial implants, etc. cause impingement between the patella bone and the bearing post during high flexion in the patients who underwent cruciate-substituting total knee arthroplasty without patella bone resurfacing. Our data showed that impingement between the patella bone and bearing post was more common in patients with mobile bearing, a small-size femoral component, and long patella or a large inferior pole angle.
Grigoris et al.6) reported that patellotibial impingement occurred owing to vertical implant design of the bearing post. Kramers-de Quervain et al.7) reported that fat pad impingement occurred less frequently in rotating platform or meniscal bearing designs than in the AP Glide (DePuy, Leeds, UK) bearing system, which was attributed to less anterior translation of the bearing. In this study, correlation between the bearing implant designs and the occurrence of impingement was observed. Impingement occurred in 90 of the 94 cases in which mobile bearing was used, while impingement occurred only in the 47 of the 124 cases in which fixed bearing was used; impingement incidence was more common in patients with mobile bearing that was relatively more anteriorly located and those with a longer post than in those with a fixed bearing (p = 0.04) (Tables 1 and 2, Fig. 3).
Verborgt and Victor9) reported that post impingement was significantly associated with a raised joint line; the mean change in the joint line position was increased by 6 ± 2 mm in the group with impingement; whereas only a + 3 mm change was noted in the group without impingement. Tang et al.13) measured the joint line in a Chinese population using magnetic resonance imaging and reported the mean distance of 11.99 ± 1.20 mm from the reference point, the fibular head, to the lateral tibial plateaus (the joint line). However, in our study, the preoperative mean distance from the fibular head (the reference) to the midpoint (the joint line) of the lateral knee joint gap was 14.0 mm and the postoperative mean distance to the lowest point (the joint line) of the lateral femoral component was 13.0 mm following total knee replacement (TKR). We were unable to confirm the correlation between changes in the joint line and impingement occurrence (p = 0.069), because the impingement occurred in 39 of the 81 cases in which the joint line decreased after surgery, as compared to that before surgery.
Verborgt and Victor9) reported a significant positive correlation between the Insall-Salvati ratio and the angle of impingement; in addition, they found a significant positive correlation between a smaller femoral component size and the point at which impingement occurred. In this study, there was no significant correlation between impingement and changes in patella bone location (p = 0.51). However, our data showed that impingement occurred more frequently in patients with a smaller femoral implant size, with a significant correlation between impingement occurrence and a smaller size femoral implant (p = 0.01).
Grigoris et al.6) also reported patellotibial impingement in patients with joint line elevation < 10 mm, in which greater flexion resulted in more forward displacement of the patella. In the present study, impingement between the lower portion of the patella and the bearing post caused forward displacement of the patella, which caused stretching of the patellofemoral ligament and retinaculum and thus reduced the flexion gap.
Kramers-de Quervain et al.7) reported that when subjects performed flexion following TKR by the LCS AP Glide bearing system, 13 cases (5.7%) complained of anterior knee pain from fat pad impingement due to narrowing of the space between the anterior edge of the AP Glide bearing and the patella ligament or the distal patellar pole. Macule et al.8) found inflammatory infiltration in the Hoffa's fat pad in 36% of the 68 TKR patients, and suggested that fibrosis of Hoffa's fat pad may cause postoperative pain and decreased range of motion.
In patients with > 45 mm patella length or > 38° patella inferior pole angle, impingement can be treated by simple resection of the lower portion of the patella. Impingement between the lower portion of the patella and the bearing post caused forward displacement of the patella, leading to stretching of the patellofemoral ligament and retinaculum and reduction in flexion gap; hence, it is possibly the cause of postoperative pain and reduction in range of motion. Since resection of the lower portion of the patella widens the space between the patella and the bearing post, it may prevent impingement between the bearing and soft tissue or the patella (Figs. 4 and 5).
Limitation of this study was the difficulty in setting the reference line for measurement due to severe osteophytes in the patella bone preoperatively. Hence, radiologic measurement shows slight individual-based differences. Another limitation of this study was the lack of measure of forward patella displacement after impingement state despite the observed forward patella displacement.
Finally, in the cruciate-substituting high-flexion total knee arthroplasty, impingement between the patella bone and bearing post was more common in patients with mobile bearing, a small-size femoral component, and a long patella or a large inferior pole angle. In cases of intraoperative impingement between the patella bone and the bearing post, resection in the lower portion of the patella prevented impingement of the bearing with soft tissue or the patella by widening the space between the patella and the bearing post, which in turn prevented postoperative reduction in range of motion.



 XML Download
XML Download