

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Facial asymmetry, defined as a difference in size between the left and right hemifaces, is a natural phenomenon1 that is caused primarily by mandibular asymmetry.2 The etiology of mandibular asymmetry is multifactorial,3 including genetic or congenital malformations such as cleft lip and palate.4
The development of mandibular asymmetry in unilateral cleft lip and palate (UCLP) patients may be caused by the following etiologic factors:5 (1) true skeletal mandibular asymmetry, (2) positional adaptation of the lower jaw to asymmetric mandibular fossae, and (3) functional adaptation to dentoalveolar and occlusal disharmonies. In the literature, some authors report significant mandibular asymmetries in cleft lip and palate patients,5,6 whereas others have found no such asymmetry.7,8
A number of tools have been used to assess mandibular asymmetry, including clinical examination; frontal- and side-view photographs; and 2-dimensional (2D) radiographs, such as lateral and posteroanterior cephalograms, oblique radiographs of the mandible taken at 45°, and panoramic radiographs.9,10 These 2D radiographs can be misleading, since complex 3-dimensional (3D) structures are projected onto flat 2D surfaces, creating distortion and magnification errors.11,12
Cone-beam computed tomography (CBCT), a 3D imaging technique designed specifically to create images of the maxillofacial region, allows 3D reconstructions of craniofacial structures from acquired volumetric data.13 CBCT provides high-resolution images (i.e., with an isotropic resolution ranging between 0.125 mm and 0.4 mm) with short scanning times (10 - 70 seconds), and requires low doses of radiation (up to 15 times lower than that of medical computed tomography scans).14 CBCTs therefore provide an opportunity for multiplanar imaging and assessment of 3D information.
However, whereas many researchers have used 2D radiographs to assess mandibular asymmetry in cleft lip and palate patients,5-7 few have used 3D imaging to investigate this phenomenon. Indeed, we could find no published studies that have evaluated mandibular asymmetry in cleft lip and palate patients using CBCT. Therefore, we undertook this study to determine (1) whether there are any differences in mandibular measurements between the cleft and non-cleft sides of UCLP patients or the right and left sides of control patients; and (2) whether there are any significant differences in mandibular asymmetry between UCLP and control patients.
MATERIAL AND METHODS
We examined the CBCT scans of 15 patients (8 males and 7 females) with UCLP (8 right and 7 left; mean age: 21.2 ± 2.1 years, range: 17.3 - 24.4 years) and 15 control patients (mean age: 22.6 ± 3.2 years, range: 17.1 - 25.2 years) that were selected from the archives of the Oral and Maxillofacial Radiology Department of Faculty of Dentistry, Dicle University. The CBCT scans were taken as part of a set of clinically necessary radiographs. Therefore, patients were not unnecessarily subjected to additional radiation, and consequently ethical committee approval was not needed. All patients attending the dental clinic of Dicle University sign an informed consent form indicating their agreement to CBCT scans.
We used CBCT scans from patients without cleft palate as controls. These patients were matched by age and gender to the UCLP patients in the study. Selection criteria for both cleft and control patients are provided in Table 1. Only cases of complete UCLP were included in the present investigation because individuals with UCLP have unilateral malformation, allowing us to use the measurements of the contralateral non-cleft side of each individual as an internal control.15 We included patients with non-significant facial asymmetry in order to evaluate isolated asymmetry of the mandible in UCLP individuals.
Facial asymmetry was determined by the degree of menton deviation (MD) from the midsagittal reference line, as defined by Grummons and Kappeyne van de Coppello.17
All CBCT images were acquired using an iCAT 3D imaging device (Imaging Sciences International, Hatfield, PA, USA), set at 5.0 mA and 120 kV. Scans with a voxel size of 0.3 mm were made with a single 360-degree rotation, 9.6-second scan. According to routine image exposure protocol, patients' heads were oriented by adjusting the Frankfort plane parallel to the horizontal plane, lateral scout radiographs were taken, and small adjustments were made. This ensures inclusion of all areas of interest and minimizes head orientation errors.
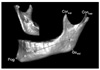
For better evaluation and a precise 1-to-1 ratio, measurements of anatomic surface landmarks and reconstructed 3D models of UCLP patients were used in this study. DICOM files obtained from the CBCT scans were reconstructed using Mimics 10.0 (Materialise NV, Leuven, Belgium). This software allows the use of both Hounsfield and gray values to separate the area of interest from its surrounding structures, enabling the visualization of areas that are superimposed by other structures in the intact model. One important structure in the diagnosis of facial asymmetry, the condyle, can be evaluated separately after the mandible has been isolated from the rest of the image.11 We used the auto-segmentation function of the software to isolate the mandibles from the images and removed the teeth above the alveolar bone of the mandibles. All landmark identifications and measurements were made using the Mimics 10.0 software. We used the landmarks described by You et al.18 in their examination of asymmetric mandibles based on condylar, coronoid, angular, body, and chin units (Table 2). These authors used the mandibular and mental foramina as important reference points at the junction of the skeletal units. Point F was proposed as a good reference point for the mandibular and mental foramina in 3D images of the mandible19 (Fig 1). Because primary intramembranous ossification begins in the mental foramen, it is generally accepted as a good point for the division of the mandibular corpus into body and chin units.18 Therefore, we used point F as a guide to measure the skeletal unit lengths.
All linear measurements were performed by controlling the localization of the landmarks in all dimensions on the reconstructed 3D surface models. The following bilateral measurements were made (Figs 1, 2, 3, Table 2): (1) condylar unit length: Consup - F; (2) coronoid unit length: Corsup - F; (3) angular unit length: F - Gomid; (4) body unit length: F - MF; (5) chin unit length: MF - Pog; (6) condylar width: Conmed - Conlat; (7) ramal height: Consup - Gomid; (8) body length: Gomid - Me; (9) hemi-mandibular volume: the mandibular volume was divided into 2 hemi-mandibular volumes by the plane connecting Me, B, and G; and (10) ramal and body volumes: hemi-mandibular volume was divided into ramal and body volumes by the plane connecting Gomid, Jlat and Jmed. In addition, the surface area of all mandibular parts was calculated. All data were measured in cm2 or cm3, and all landmark identifications and measurements were made by one individual to prevent interobserver variability.
To determine the errors associated with CBCT measurements, 15 of the CBCT images were randomly selected and re-measured 4 weeks after the initial measurements.
Statistical analysis
All statistical analyses were performed using the statistical package for social sciences, 13.0 (SPSS for Windows; SPSS Inc., Chicago, IL, USA). Normality of the data was tested using Shapiro-Wilks tests, and the homogeneity of variances was verified using Levene's test. All UCLP and control patient asymmetry data was normally distributed with homogeneous variance, except for gender data. Therefore, we used parametric tests to evaluate the asymmetry data.
Wilcoxon tests were used to compare genders. To compare the measurements between the cleft and non-cleft sides in UCLP patients, and the right and left sides in control patients, we used paired-sample t-tests. We performed independent t-tests to evaluate sideto-side differences and differences between cleft and control patients. To evaluate the differences in asymmetry between control and UCLP patients, we compared the right-left differences of controls with the cleft-non-cleft differences of UCLP patients. p-values less than 0.05 were considered significant. Results are reported as the means ± standard deviations.
RESULTS
A Bland and Altman plot revealed no significant differences between repeated measurements of the same radiograph (Table 3). There were also no significant differences between any of the median measurement values for male and female subjects (p > 0.05 for all). Therefore, data for both genders were pooled for further analyses.
Descriptive statistics and comparisons of the linear, surface, and volumetric measurements between the cleft and non-cleft sides of UCLP patients are presented in Table 4. In UCLP patients, the coronoid unit was longer on the cleft side (p = 0.046). This was the only significant difference between the cleft and non-cleft sides of these patients. Only the ramal height (p = 0.024) and body length (p = 0.021) were significantly different on the right and left sides of control patients (Table 4). Therefore, the data for both sides in each group were pooled for further statistical analysis.
Comparison of measurements between groups indicated that the body volume was significantly lower in UCLP patients than in controls (16.08 ± 4.99 cm3 vs. 20.56 ± 3.35 cm3; p = 0.008; Table 5). Comparison of the differences between the cleft and non-cleft sides of UCLP patients with the differences between the left and right sides of control patients indicated that side-to-side body length differences were greater in the control group than in the UCLP group (p = 0.032), whereas side-to-side differences in chin unit length and hemi-mandibular surface area were greater in the UCLP group than in the control group (p = 0.019 and p = 0.044, respectively; Table 6).
DISCUSSION
In UCLP patients, facial and nasomaxillary skeletal asymmetries are commonly present with the nasomaxillary complex being more asymmetric in affected individuals than in non-cleft controls.20 Previous 2D studies on facial asymmetry have reported that the mandible appears to be the leading factor in facial asymmetry. 21,22 Because quantitative measurement is a key element in the diagnosis of asymmetry, 3D structures cannot be properly analyzed with 2D radiographs.11 We therefore used 3D images to assess mandibular asymmetry in cleft lip and palate patients.
Previous studies have shown that UCLP patients reach the postpubertal growth spurt at a later age than do non-cleft patients.23 da Silva Filho et al.24 reported that cleft patients, irrespective of the type of cleft, have smaller mandibles than non-cleft patients at adulthood. Krogman et al.25 used postero-anterior cephalometric radiographs to assess craniofacial growth and noted a significantly larger gonial height in the UCLP group and bilateral CLP group during early and late childhood. Further, Laspos et al.26 studied postero-anterior radiographs of children and reported that UCLP patients had mandibles that were more asymmetric than those of controls. In contrast, Athanasiou et al.27 found that those children with cleft palates who have undergone corrective surgery may have normal growth rates. In the current study, only post-adolescent patients were included to eliminate possible growth rate differences. We are therefore unable to discuss the cause-and-effect relationship between mandibular asymmetry and growth.
Liukkonen et al.1 reported that facial asymmetry is a natural phenomenon often due to differences in mandibular dimensions on the right and left sides. They also concluded that healthy young subjects generally have some degree of mandibular asymmetry. In the present study, side-to-side comparisons of control patients revealed statistically significant differences in ramal height and body length. We attribute the differences in these measurements to natural asymmetry. On the other the hand, the side-to-side comparison in the UCLP group revealed that the coronoid unit length was significantly longer on the cleft side. The coronoid unit is affected by the temporalis muscle28; however, sideto-side comparison of temporalis muscle volume revealed no statistical difference in patients with facial asymmetry.29 It is difficult to attribute the difference in coronoid unit length directly to muscular activity because the muscles and other soft tissues were not considered in the current study.
Side-to-side differences in chin unit length, body unit length, and hemi-mandibular surface measurements were significantly different between the groups in this study. However, no statistically significant differences were found in any of the other measurements considered. These differences may be related to genetic factors or to functional activity of the skeletal muscular system, particularly in the masticatory apparatus.
According to Laspos et al.,5 UCLP patients may have cranial base/temporal region anomalies that are responsible for asymmetry of the lower facial skeleton. Smahel and Brejcha6 studied the lateral and PA radiographs of 58 UCLP patients (32 complete CLP and 26 incomplete clefts of the palate) and found no significant differences between the two cleft groups, except for a shorter mandibular ramus in complete UCLP patients. Smahel and Mullerová30 used lateral and posteroanterior radiographs to study the craniofacial morphology in UCLP patients prior to palatoplasty and detected significant shortening of the mandibular body and ramus. In contrast, Horswell and Levant investigated 16 complete UCLP patients and found that the mandible was normal in every dimension.31 Kurt et al.7 compared the condylar, ramal, and condylar plus ramal height values on panoramic radiographs and found no statistically significant differences except gonial angle, and they considered that this difference might result from a compensation mechanism of the mandible on the cleft side. In the current study, only body volume was significantly different between cleft and non-cleft patients. We attribute the differences between our results and those of earlier studies to the use of different research methods and landmarks used for assessment. Additionally, differences in body volume may result from muscular activity and functional adaptation to soft tissue disharmonies. However, these were not considered in the present study. Further study is needed to understand the role of soft tissues, including muscle volume and muscle activity, in the observed mandibular asymmetry in UCLP patients.
One limitation of this study is the small sample size. To overcome this limitation, patients' age and gender were homogenized, and the same author carefully performed all measurements. The high precision of CBCT quantitative analyses contributes to the reliability of the measurements rendering small sample sizes acceptable.32 Future studies with large sample sizes are needed for further explore facial asymmetry in UCLP patients.
CONCLUSION
Mandibular asymmetry was evaluated 3-dimensionally using the CBCT data of UCLP patients. From this evaluation, we conclude the following:
1. There is no statistically significant difference between genders in mandibular asymmetry measurements
in either group.
2. In the UCLP group, coronoid unit length was significantly longer on the cleft side than on the non-cleft side. Only ramal height and body length were significantly different between the left and right sides of non-cleft control subjects.
3. Although body volume was larger in UCLP patients than in controls, both groups had similarly symmetrical mandibles.








 XML Download
XML Download