

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Since the introduction of miniscrews for orthodontic anchorage, various tooth movements that had been previously thought impracticable are now considered possible. For example, the skeletal open bite, which has been corrected with combined surgery of the maxilla and mandible, can be treated with miniscrews without orthognathic surgery.1-3 Recently, it was reported that space can be gained by molar distalization with miniscrews a non-extraction treatment.4-6 Although the treatment results with miniscrews are remarkable, this treatment raises challenges not encountered before.
Among these, frequent loosening is one of the main challenges that needs to be overcome. The osseointegrated dental implant used to restore missing teeth has undergone various modifications to increase the success rate, such as changes in diameter, length, pitch, and thread shape.7,8 However, efforts to enhance the stability of orthodontic miniscrews with design modifications have just begun. One approach is to place a tapered miniscrew based on the assumption that the tapered shape might affect initial stability.9,10 The tapered shape pushes out the bone around it as it is inserted, inducing compressive pressure on the cortical bone around the neck where the stress is mainly concentrated when elastics are applied.11 The effect of a tapered shape can be considered an advantage or disadvantage in terms of stability. It is an advantage if it increases the bone density around the neck, enhancing stability.10,12-14 However, it is a disadvantage if it causes excessive pressure, sufficient to inhibit blood flow to the osteocytes within the bone, leading to cell death and bone necrosis.15
Another way of increasing miniscrew stability is to wait 2 - 4 weeks for osseointegration. Animal studies16,17 suggested that miniscrews might undergo osseointegration. However, some studies recommend placing a load immediately without waiting for healing.10,18-20 Moreover, studies revealed no significant differences between the groups of delayed loading and immediate loading.21-24
This study compared the stability, as determined by torque values, of a cylindrical miniscrew with that of a tapered one in order to determine if the tapered shape enhances miniscrew stability and to determine if the healing time before loading affects the stability of the miniscrew. We also aimed to determine if the insertion torque is associated with the removal torque, which is measured after a few weeks of healing.
MATERIAL AND METHODS
This study was reviewed and approved by the Institutional Animal Care and Use Committee (IACUC) of Samsung Biomedical Research Institute (SBRI). The SBRI is an Association for the Assessment and Accreditation of Laboratory Animal Care International (AAALAC International) accredited facility and abides by the rules of the Institute of Laboratory Animal Resources (ILAR) guide.
Miniscrews
Two types of miniscrews, tapered and cylindrical, were made from BMK (Orthoplant, Biomaterials Korea Inc., Seoul, Korea) so that they generated similar maximum insertion torque values (ITVs), as determined by preliminary studies performed on artificial bone blocks. This was possible because the tapered design had a higher torque value than the cylindrical design,25 even if the thread lengths differed. The thread length of the cylindrical miniscrews (Cy) was 7 mm. Cy are the most popular orthodontic miniscrews on the market. The tapered miniscrews (Ta) had a thread length of 5 mm; tapering was more than usual in order to amplify the effect of this shape (Fig 1).
Animals and anesthesia
Twelve female New Zealand white rabbits (body weight: 3.0 - 3.5 kg) were used in this study. The rabbits were anesthetized with xylazine (5 mg/kg administered intramuscularly) and ketamine (35 mg/kg administered intramuscularly). Next, 1 ml of 2% lidocaine was injected into the surgical regions of the tibia for additional local anesthesia.
Measurement of maximum insertion torque value (ITV)
Prior to surgery, the regions to be operated upon were shaved and decontaminated with iodine and 70% ethanol. The tibia was exposed by incising through the skin, fascia, and periosteum. Although the miniscrews were drill-free types, a preliminary study found that tibia fractures occasionally occurred without pilot holes when the miniscrews were inserted; the fractures were attributed to the cortical bone of the rabbit tibia being too hard. Pilot holes with a 1 mm diameter were drilled at 30 rpm, using a bone drill on the body of the tibia under saline irrigation to minimize the amount of heat. The distance between the 2 holes was approximately 15 mm. Two types of miniscrews, Cy and Ta, were placed only until the upper ends of the thread were flush with the external surfaces of the tibia bone (Fig 2). In other words, 5 mm and 7 mm of thread in the Ta and Cy, respectively, was inserted into the bone. Two Cy were placed on one side of the 2 legs, and 2 Ta were placed on the other side. ITV was measured using a digital torque driver (DI-5-RL2; Sugisaki Meter Co., LTD 5085-23, Ibaraki, Japan) in Ncm units (Fig 3). No orthodontic forces were applied in order to observe the pure effects of the different designs. Surgical sites were closed in layers. The muscle, fascia, and internal dermal layers were sutured, while the outer dermis was sutured for primary closure. After surgery, all rabbits were administered the antibiotic, Baytril, at a dose of 10 mg/kg and ketoprofen at a dose of 1 mg/kg.
Measurements of maximum removal torque value (RTV)
There were 3 groups of 4 rabbits each. Rabbits were grouped according to the healing period (2, 4, and 6 weeks). Four rabbits were sacrificed at the end of each healing period. The maximum RTVs were obtained while the rabbits were still alive in order to reproduce the clinical situation. The rabbits were anesthetized with an intramuscular injection of ketamine (35 mg/kg) and xylazine (5 mg/kg). The maximum RTV was measured using a digital torque gauge (Fig 3) and recorded. After confirming the RTV, the anesthetized rabbits were euthanized using KCl.
Statistical analysis
For comparisons between the 2 types of miniscrews and between groups, due to small sample size, median regression adjusting for location, type of miniscrew, healing period, and subject was used. p-values were corrected using Bonferroni's method, adjusting for inflated type I error. The correlation between ITV and RTV was also tested using median regression, adjusting for type, location, and healing periods. A p-value of <0.05 was considered significant.
RESULTS
All rabbits recovered from the anesthesia without complications, and all miniscrews were found to be stable at the end of the 3 experimental periods. Upon re-exposure, some of the miniscrews were partially covered with bone. The bone over the head of the miniscrews was removed with a scalpel before measuring the RTV with a torque gauge in order to avoid biased values.
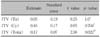
There was no significant difference between Ta and Cy in terms of the median ITVs or RTVs within each group. The median (Q1-Q3) total ITV in Ta and in Cy were 15.8 (10.7 - 23.5) Ncm and 15.6 (10.4 - 24.0) Ncm, respectively, and the median (Q1-Q3) total RTV in Ta and in Cy were 5.3 (4.3 - 7.6) Ncm and 5 (3.9 - 7.9) Ncm, respectively. Analysis using median regression adjusting for location and healing time effects showed that the difference between Ta and Cy was not significant in terms of total ITV (p = 0.68) and total RTV (p = 0.41) (Table 1).
DISCUSSION
Torque is closely related to the factors that determine the stability of miniscrews, such as bone density26,27 and cortical bone thickness.28 In addition, the torque value is frequently used as an indirect method to assess the stability of an implant or miniscrew.9,29-32 There are 2 types of miniscrews available: tapered and cylindrical. However, there is limited information about their differences.
Lim et al.33 reported that there was a significant increase in insertion torque with increasing screw diameter. There were no significant differences in the total ITV and RTV between Ta and Cy as well as in the ITV and RTV within each group (Table 1). The similar ITV was intended from the study design and meant that the experimental procedures had been carried out appropriately.
The length and diameter are 2 major factors that determine the stability of a miniscrew.34,35 The median (Q1-Q3) RTV of Ta [5.3 (4.3 - 7.6) Ncm] was comparable to that of Cy [5 (3.9 - 7.9) Ncm]. The RTV of Ta should be lower than that of Cy if bone cells are injured as a result of too much pressure originating from the tapered shape. However, Ta and Cy showed similar stability, even though Ta were 2 mm shorter than Cy. This stability was attributed to the similar diameter of the two types at the level of the cortical bone, which is believed to provide the miniscrews with the main mechanical retention. Ta might not cause excessive pressure to the bone tissue, and they induce a similar bone reaction to Cy. The shorter shank of Ta could be advantageous over Cy because the proximity of a miniscrew to the root is a major risk factor for the failure of screw anchorage.21 The longer thread of Cy increases the likelihood of root contact. Therefore, Ta could be more advantageous in terms of less root damage and better stability. Although the tapered shape increased the crestal strain,7 some in vitro13,25 and animal studies9,10 have reported that the tapered design is more advantageous than the cylindrical design in terms of mechanical and biological stability.
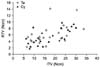
Some orthodontists load the miniscrew immediately, whereas others do not. The waiting period before loading varies according to the clinician. Therefore, it is necessary to determine which of the 2 loading protocols is more beneficial for miniscrew stability, and how long a waiting period is appropriate if delayed loading is better. Early loading might decrease the level of osseointegration of orthodontic mini-implants.17 Some studies suggest that the machined surface of pure titanium or titanium alloy could be integrated with bone.30,36 However, other researchers20-24 could not find any influence of a waiting period before loading on the stability of orthodontic miniscrews. These results are in accordance with those of the present study. which found no differences between the mean RTV of the 3 groups, suggesting that no osseointegration occurred with time. Roberts reported 6 weeks to be an adequate healing period in rabbits prior to loading in order to attain rigid stability.37 If osseointegration progresses with healing time, the RTV in this study would increase with time, as reported by Klokkevold et al.30 However, the RTV in this study was similar in all the 3 groups (Table 1), which is consistent with some studies.18,24 According to Morais et al.,16 who examined rabbits, there was no increase in the RTV when the healing period was between 1 and 4 weeks. However, the RTV increased significantly after 12 weeks. In the present study, the 5 miniscrews circled with a red line in Fig 4. showed relatively higher RTVs than ITVs as compared with the other miniscrews. Four out of the 5 miniscrews were included in the group that was allowed a healing period of 6 weeks, and the remaining one was from the 4-week group, which strongly suggests integration between the bone and miniscrews. Therefore, orthodontic miniscrews with a machined surface of Ti-6AI-4V titanium alloy could be integrated with bone experimentally, as reported in Morais' study.16 On the other hand, a healing period of more than 6 weeks to improve the stability of miniscrews is unsuitable for orthodontic patients. The results of other studies and the present study suggest that it would be difficult to obtain osseointegration in humans within a few weeks. Therefore, it is not recommended to wait for a few weeks before applying a force, expecting better fixation of the miniscrew. The orthodontic miniscrew is not made primarily of pure titanium. Moreover, it is not surface-treated or packed as a prosthetic dental implant, and the entire placement procedure differs from that of a prosthetic dental implant. Placing a low-intensity load immediately after placing early orthodontic static loads did not affect the mini-implant's performance.38
There have been no objective references to determine the future stability of a miniscrew. Clinicians are only able to presume its stability on the basis of the resistance carried to their hands through the driver handle. Although Resonance Frequency Analysis (RFA),39-41 periotest,42 and insertion torque26,40 measurements are used to assess the stability of an osseointegrated prosthetic implantor miniscrew, none of these are the gold standard. The RTV is closely related to the stability of miniscrews rather than to the ITV because it reveals the degree of fixation that has occurred after the bone reactions that occurred during healing. Median regression adjusting for time, type, and location effects revealed a correlation between the ITV and RTV (p = 0.022), which means the RTV increased with the ITV. There was, however, no significant correlation between each tapered and cylindrical miniscrew. Scatter plots for Ta and Cy demonstrated similar patterns (Fig 4). The reason, therefore, for significant correlation between the ITV and RTV in 48 miniscrews seemed to be the large sample size. It was presumed that ITV might be an indicator of the future stability of a miniscrew. This is not consistent with the results obtained by Motoyoshi,11 who reported that the optimal placement torque to raise the success rate of a mini-implant ranges from 5 to 10 Ncm. and Okuyama43 in accordance with Ottoni et al.44 reported that the potential risk decreased with increasing ITV, and Song et al.25 who stated that the RTV increases as the ITV increases.
This study had some limitations. The first was that the healing time appeared to be too short to observe all the changes occurring at the interface between the miniscrew and bone, even though a 6-week healing period in rabbits is equivalent to approximately 18 weeks in humans.37 The second was that this study did not determine if the stability of miniscrews varied with design in the case of force application. Third, a histomorphologic analysis should have been performed to compare the precise differences in bone reactions to Ta and Cy.
CONCLUSION
The shorter Ta showed similar stability to the Cy, which strongly suggests that the tapered shape is more advantageous than the cylindrical shape.
RTV did not increase significantly over time. It is recommended that a miniscrew be loaded immediately; waiting a few weeks before loading should be avoided.
There was a correlation between the ITV and RTV, indicating that the ITV can be used as an indicator of the future stability of a miniscrew.




 XML Download
XML Download