

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Gallbladder torsion is a rare condition requiring urgent cholecystectomy for a gangrenous change of the gallbladder. Elderly women are most commonly affected with this condition as the number of reports has been recently increasing with aging population.12 Anomalous attachment of the gallbladder to the liver with long or absent mesentery is the most common cause of gallbladder torsion. Age-related laxity of tissue may be another predisposing factor of this disease. The most common anatomical variants include a floating gallbladder with a long and short mesentery containing cystic artery and cystic duct.3 However, a different mechanism may underlie gallbladder torsion. The present study reports of a rare type of gallbladder torsion, in which the fundus of the gallbladder was rotated counterclockwise along the axis near the end of mesenteric attachment of gallbladder to the liver. A strong peristaltic movement of the colon may precipitate the torsion of gallbladder fundus, which is not firmly attached to the liver. Only four cases of such gallbladder torsion, which underwent surgery, have been reported in the literature.4567 This study presents a case in which fundus rotate along the axis of gallbladder.
CASE
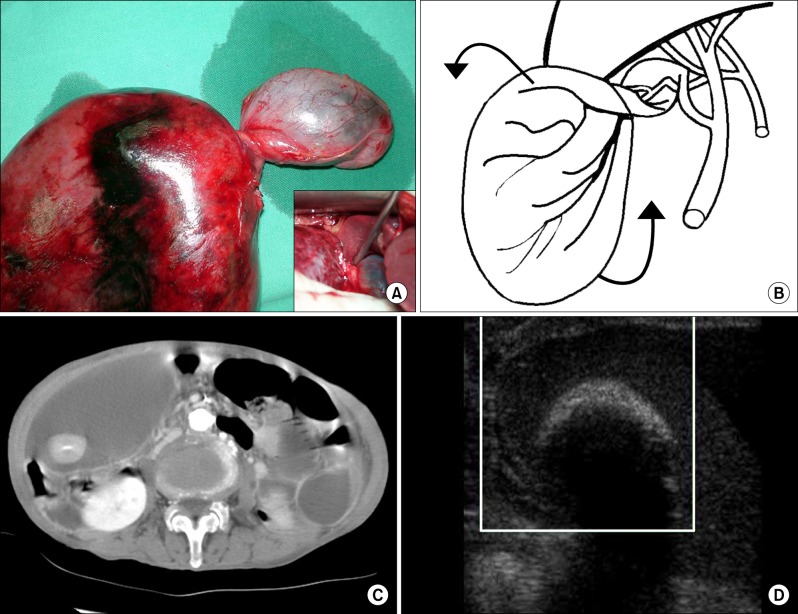
An 87-year-old woman complaining of abdominal pain in the right upper quadrant, nausea and vomiting for 4 days was admitted to the emergency room. She was moderately dehydrated with fever (38.5℃) but her vital signs were normal. On physical examination, a large, firm and tender mass was palpable on the right abdomen. Her conjunctiva was not icteric. Liver function test was normal. Computed tomography of abdomen showed a large and small cavity (Fig. 1A). The large cavity with the largest diameter of 15 cm had wall thickening and contained a large stone. The 3 cm-sized small cavity under the liver seemed to be a portion of normal gallbladder. The wall of large cavity was thickened and seemed to be the gangrenous portion distal to the twisted body of gallbladder. Ultrasonography demonstrated a portion of gallbladder rotating in a counterclockwise direction along the axis of gallbladder. Doppler ultrasonography confirmed blood flow in the small cavity proximal to the twisted portion, but there was no blood flow in the huge cavity distal to the twisted portion of the gallbladder (Fig. 1B). Gallbladder torsion was suggested preoperatively, based on the imaging findings. During laparotomy, a normal cystic duct, gallbladder neck, and proximal body was found to be attached firmly on the gallbladder bed. Moreover, the distal portion of gallbladder was twisted 360 degree in counterclockwise direction around the axis of gallbladder resulting in huge distension with severe gangrenous change of distal gallbladder (Fig. 1C). The mechanism of gallbladder torsion was illustrated (Fig. 1D). Cholecystectomy was performed and the patient was discharged 2 weeks later without postoperative complication. Histopathology showed mild inflammation found in the proximal part of the gallbladder in contrast to necrosis and gangrenous changes found in the distal gallbladder.
DISCUSSION
Gallbladder torsion results in acute gangrenous cholecystitis requiring urgent cholecystectomy. Although, gallbladder torsion may occur in all ages, it is an elderly disease. Age-related weight loss and visceroptosis may be etiologically related to gallbladder torsion.2 Female patients are more commonly affected than male, with the female to male ratio of 3 : 1.1 Once complete torsion occurs, the patient suffers from acute upper right quadrant pain that mimics acute cholecystitis. Due to the lack of specific symptoms and signs, it is rarely diagnosed preoperatively based on clinical findings. However, recently, with the advances of imaging diagnosis, several reports of preoperative diagnosis of gallbladder torsion have been published. The lack of blood flow by the duplex ultrasonography was helpful in the diagnosis.8
Marano et al.3 described three anatomic variants of gallbladder attachment to liver responsible for gallbladder torsion. The first variant is a "free-floating gallbladder" suspended only by the mesentery of cystic duct. The gallbladder rotates around a vascular axis represented by the cystic artery and duct. The second variant is elongated, narrow-based and freely mobile mesentery and rotation occurs along the axis of the narrow mesentery. An exceedingly rare third variant consists of a normally fixed gallbladder to a mobile liver lobe free of its coronary and triangular ligaments.9 In addition, to these mechanisms, as shown in our case, twisting of fundus along the axis of gallbladder body is another mechanism of gallbladder torsion.
Age-related laxity of gallbladder tissue may be a factor of the elongated fundus which rotated in a counterclockwise direction along the axis of gallbladder. A strong peristaltic movement of the colon may precipitate the counterclockwise torsion of elongated gallbladder fundus. So far, very few cases of such gallbladder torsion, which underwent surgery, have been reported in the literature.456
Only four cases of gallbladder torsion caused by this mechanism have been reported so far (Table 1). One case of the reports showed two gallbladder cavities, which were separated by the twisted portion of gallbladder on the ultrasonography, as shown in our case. In this case, normal looking proximal gallbladder that was shown in abdominal computed tomography led to confusion but ultrasonography detected the twisted portion, and this made it possible to trace the portion of twist in an anticlockwise direction. Furthermore, Doppler ultrasonography confirmed impairment of blood flow in the distal cavity whereas it demonstrated normal blood flow in the proximal cavity. Microscopic findings of the distal gallbladder wall showed infraction in the background of chronic cholecystitis compared to the relatively normal wall of proximal gallbladder. Some authors reported similar cases with intermittent torsion of the fundus, which were relieved by endoscopic retrograde cholangiopancreatography. These cases may represent an incomplete torsion of this mechanism.
Based on the gross and microscopic morphology, the study concluded that the patient had normal attachment of the gallbladder mesentery to the liver, but the elongated mobile fundus caused by age-related laxity of the gallbladder tissue and peristaltic movement of the colon precipitated the rotation of the fundus. Her accompanying gallbladder stone of 3 cm in size might be another precipitating factor for the torsion. This therefore represents a rare distinctive mechanism of gallbladder torsion.

 XML Download
XML Download