

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Hepatocellular carcinoma (HCC) is the most frequent primary hepatic malignancy.1 Hepatic resection and liver transplantation is recommended by the latest guidelines for early HCC, meeting the Milan criteria with the 5-year survival rate potentially reaching 50 to 75%.23 However, a limited number of patients can be treated with liver transplantation due to its strict indication, high cost and limited donor liver availabiity.4
Generally, anatomical hepatic resection is preferred when treating HCC because HCC has a tendency to invade the portal veins and spread along intrasegmental branches.5 Few patients however are suitable for liver resection because of poor liver function6 such as cirrhosis, chronic liver disease and the difficulty in predicting postoperative liver failure. Non-anatomical hepatic resection (NAHR) is an attractive alternative treatment option for patients with cirrhotic liver limiting resectability of liver. It has been previously reported that non-anatomical resection is equal to anatomical resection, and in some cases non-anatomical hepatic resection is recommended over anatomical resection.78 Radiofrequency ablation (RFA), which is one of the local ablative techniques, was reported to be effective in achieving complete tumor necrosis. RFA is currently used for treating resectable small HCC.9 Although the effectiveness is less well established than hepatic resection, RFA has been widely accepted for treating patients with unresectable HCC.7 RFA is an attractive treatment due to its advantages over liver resection, including a reduced destruction of normal liver tissue, lower cost, lower complication rate, and shorter hospital stay.1011 In spite of this, there is still debate over whether RFA or Hepatic resection is the most suitable therapy for small HCC. Many previous studies have compared hepatic resection and RFA, however, there is a lack of studies comparing the efficacy of NAHR and RFA.
This study aims to compare the effectiveness of RFA and NAHR, especially the short term results, for small sized HCC retrospectively.
MATERIALS AND METHODS
Procedure and indication of RFA
The indications of intraoperative RFA are as follows: tumors which were superficially located, but the patient was not indicated for liver resection due to advanced liver cirrhosis which means that the percutaneous RFA approach is not possible.; tumors which were deeply located or located at posterior surface segment 6, 7, 8 of the liver and liver resection was not indicated due to advanced liver disease and/or advanced variceal formation.
The RFA operation methods have been previously reported.9 The Cool-tip™ (18Gauge) Radiofrequency Ablation System and the Evident™ Microwave Ablation System (Covidien, CO, USA) were used. Dynamic liver Magnetic resonance imaging (MRI) was performed, preoperatively, to determine exact tumor localization, size and number. After careful liver mobilization to prevent tumor injury, the whole liver was scanned by intraoperative sonography and tumor localization performed. In the laparoscopic approach, patient position was important. A supine position was useful for anteriorly located tumors and whole liver scanning, but if the tumor was located in segment 7 or the posterior surface of segment 6 of liver, 45 degree right side up position was more useful for liver mobilization and traction during ablation. Ablation size was selected according to tumor size, was the electrode being larger than the tumor. A radiofrequency electrode was carefully inserted into the tumor and ablation was performed by the operator. In the superficially located tumor, the radiofrequency electrode was inserted into normal liver tissue to prevent tumor popup during ablation. If tumor size was larger than 2 cm, two or more ablations were performed for a larger safety zone of at least 1 cm. Single radiofrequency current was emitted for 12 minutes.
Patients
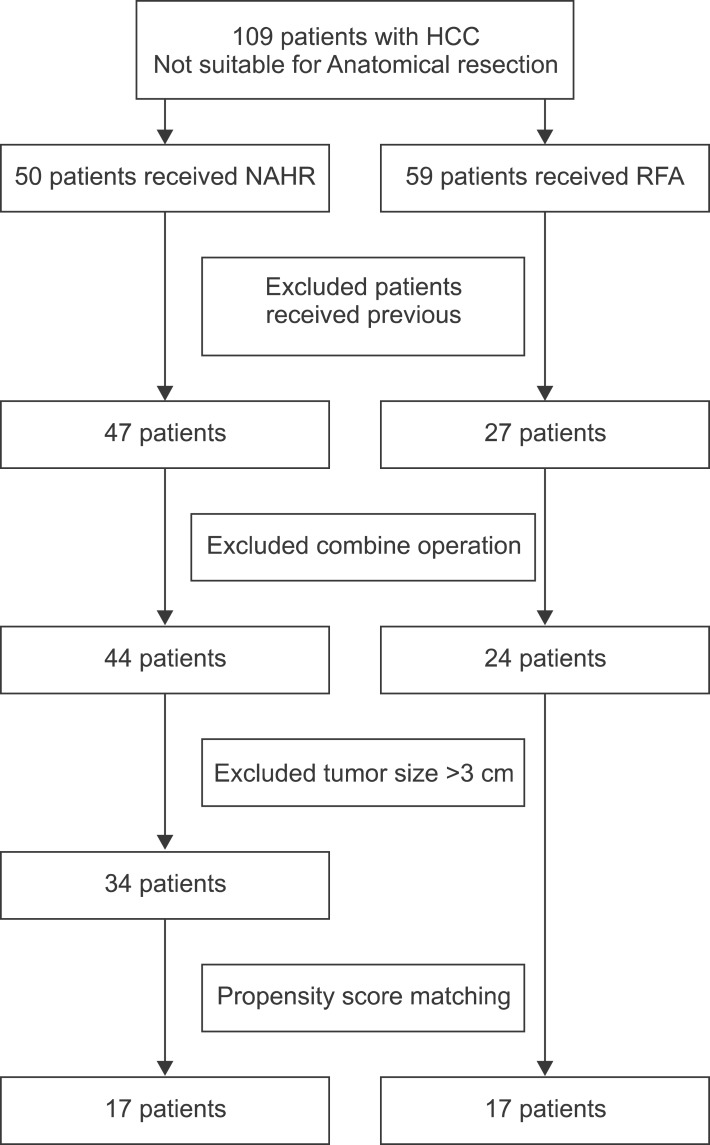
From February 2007 to January 2015, we performed intraoperative RFA on 59 patients and NAHR on 50 patients with HCC at Chungnam National University Hospital. These patients were not suitable for anatomical resection because of unfavorable ICG test results, or were candidates for liver transplantation. We excluded patients who had received any previous treatment for HCC, or liver transplantation during the follow up period. We also excluded patients who received combined operations for other disease. Small HCC was defined as a tumor size less than 3 cm whether it was single or multiple on preoperative hepatic imaging. 24 patients of intraoperative RFA and 34 patients of NAHR were enrolled in this study. Initially intraoperative RFA was indicated for patients with the worst liver function, more advanced liver cirrhosis and deep location of the tumor, when compared to those put forward for NAHR, meaning that baseline patient characteristics would be different. To overcome this, 17 pairs of matched patients were enrolled in this study by propensity score matching method (Fig. 1).
The diagnosis of HCC was based on imaging modality, including enhanced computed tomography (CT), MRI, and tumor markers. Considering cancer cell seeding during liver biopsy, preoperative liver biopsy was not suggested for all patients. Diagnosis of HCC mainly depended on typical findings; early-phase enhancement or late-phase contrast washout. Elevation of alpha-fetoprotein (AFP), history of hepatic viral infection or heavy alcohol consumption were also considered supplemental. Prior to treatment, all patients underwent basal laboratory tests including bilirubin, albumin and prothrombin activity. In terms of tumor location, a subcapsular lesion was defined as a tumor located within 2 cm from the liver capsule and segment was defined according to the Couinaud segments. Written informed consent was obtained from all patients before treatment.
Follow-up
Follow-up contrast enhanced computed tomography was performed immediately after RFA, and every three to four months in the first 2 years for every patient. For each follow up, blood tests including liver function tests and tests of serum AFP, were conducted. If HCC recurred we performed proper treatment for patients considering health status.
Statistics
All analysis was performed using the statistical software SPSS version 19.0 (SPSS Inc., Chicago, IL). Comparisons between the two groups were done using the Student's t-test for continuous data and the chi-square test for categorical data. Propensity score matching method was used for matching baseline characteristics of the two groups. The relative prognostic significance of the variables in predicting recurrence-free survival was analyzed using multivariate Cox proportional hazards regression analysis. The recurrence rate was calculated using the Kaplan-Meier method. Significant difference was considered when p<0.05.
RESULTS
Patient & tumor characteristics
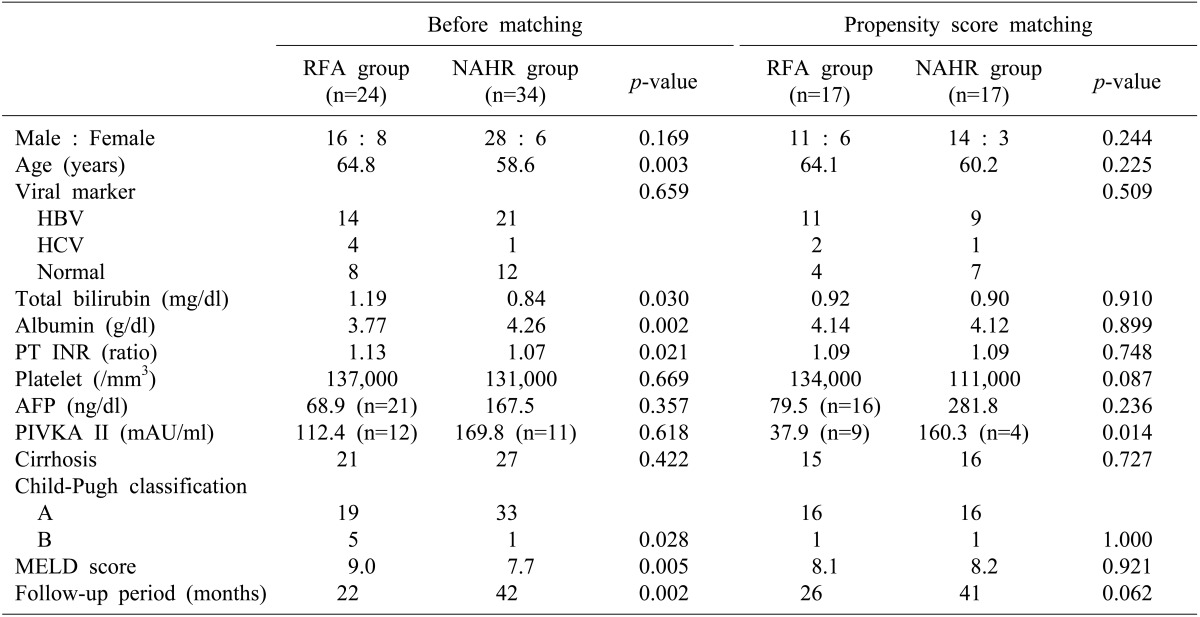
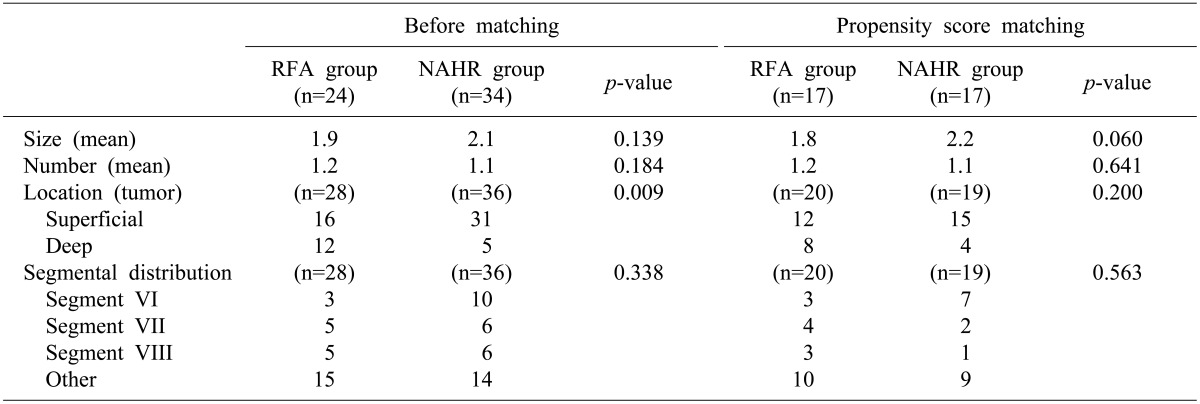
The demographics and clinical characteristic are summarized in Tables 1 and 2. The NAHR group was younger in mean ages (58.6 vs. 64.8 years; p=0.003) and had better PT INR result (1.07 vs. 1.13; p=0.021), albumin (4.26 vs 3.77 g/dl; p=0.002), and model for end-stage liver disease (MELD) score (7.7 vs. 9.0; p=0.005) than the RFA group. There was more Child-Pugh classification A in the NAHR group. There was no significant difference in sex, viral marker, cirrhosis, platelet count between the two groups. More tumors were located in the subcapsular area in the NAHR group (p=0.009) but segmental distribution were not significantly different. Mean tumor size and tumor number were not different between two group. Follow-up periods were significantly longer in the NAHR group (42 months vs 22 months, p=0.002). Baseline characteristics, in particular liver function, were different between two groups. 17 pairs of patient were selected by propensity core matching method for matching baseline characteristics between two groups. The baseline patient and tumor characteristics were not statistically different between two groups (Tables 1, 2).
Comparison of the recurrence and overall survival rates
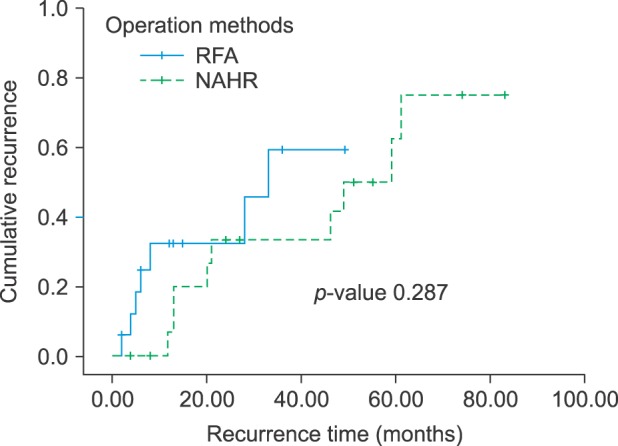
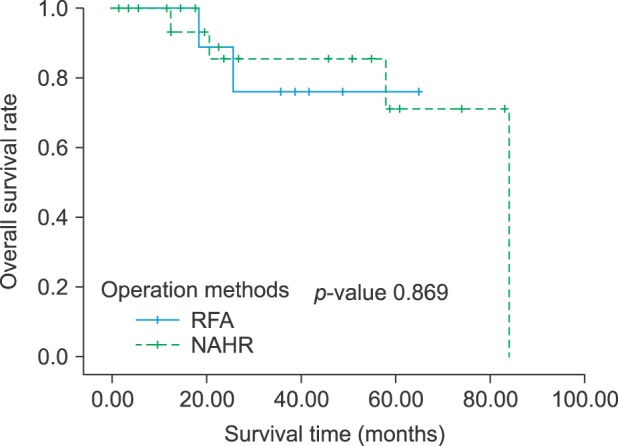
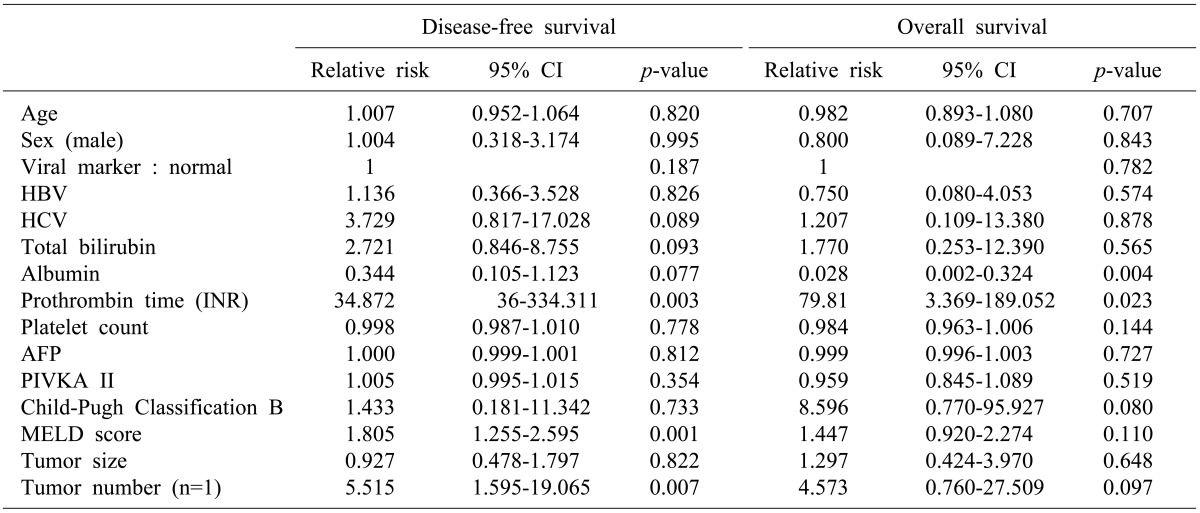
The recurrence rate at 1, 2 and 3 years were 32.2%, 32.2% and 59.3% respectively in the RFA group, and 6.7%, 33.3% and 33.3% respectively in the NAHR group (p=0.287) (Fig. 2). In univariate analysis, PT INR, MELD score, and tumor number were predictors of tumor recurrence (p=0.003, p=0.001, p=0.007, respectively) (Table 3). In multivariate analysis, tumor number was a predictor of recurrence (p=0.019) (Table 4). The OS rates at 1, 2 and 3 years were 100%, 88.9% and 76.2% respectively in the RFA group, and 100%, 85.6% and 85.6% respectively in the NAHR group (p=0.869) (Fig. 3). In univariate analysis, albumin and PT INR were predictors of overall survival (OS) (p=0.004 and p=0.023, respectively) (Table 3). In multivariate analysis, albumin was a predictor of recurrence rate (p=0.020) (Table 4).
DISCUSSION
HCC is the most frequent primary hepatic malignancy and, with the advance of diagnostic imaging modality, the diagnosis of small HCC has improved considerably. It has allowed patients to have the opportunity to cure HCC by hepatic resection or local ablation, for example using RFA.11213 However, many clinicians find it difficult to select the optimal therapy and treatment for individual patients with HCC. Although hepatic resection is considered the treatment of choice for HCC, many factors, including liver dysfunction, general condition of the patient and tumor location, and portal vein invasion of tumor, often limit the indication for hepatic resection and extent of treatment.1415 Under such circumstances, NAHR or RFA could be appropriate treatments for small sized HCC.
To date there has been no study comparing NAHR and RFA to determine which is the better treatment for patients with small HCCs. Several randomized controlled trials (RCT) have compared the efficacy of hepatic resection and RFA. Imai et al. concluded that in 2-3 cm HCC, hepatic resection would be the first-line therapy because of an observed higher survival rate and lower recurrence rate.16 Wang et al.17 reported that for HCC patients in the BCLC very early/early stage, surgical resection yielded better disease-free survival rate than RFA. However, in these RCTs, non-anatomical hepatic resection and anatomical hepatic resection, and percutaneous RFA and intraoperative RFA, were not distinguished. In our study, we compared the survival rates between NAHR and intraoperative RFA in patients with HCC less than 3 cm. Of course these patients were treated with the intension to treat.
In this situation, the different recurrence rates between the two groups could be related to differences in background characteristics, especially liver function related factors. The result of high recurrence and low OS rate in the NAHR may be the result of liver function, as liver function is related to liver fibrosis, and liver fibrosis is associated with a high risk of multi-centric carcinogenesis.18 As such prothrombin activity, albumin, total bilirubin, and Child-Pugh class could be the strongest predictors.1920212223242526 To equalize these variables of the two groups, we used the propensity score matching method. In this study, OS and recurrence rates of NAHR surpassed those of intraoperative RFA group, except after 2-years when OS and recurrence rates were not significantly different between the two groups. This result may be explained by initial small scale cohorts.
Tumor recurrence post-RFA differed from post-liver resection that makes sufficient safety margin. In immediate postoperative state, RFA area could be confirmed via a comparison of before and after CT scan, but this imaging may not be sufficient for defining tumor necrosis and sufficient margin27 because of mobilization during intraoperative manipulation. As such, some RFA results could cause misinterpretation of complete ablation. Tumor pop-up is another key problem. Superficially located tumors that are directly punctured can pop-up though the needle hole. This complication could be a source of peritoneal drop metastasis but can be easily prevented by puncturing though normal tissue and capping the tumor with surgical gauze. These tumor pop-ups could also cause tumor spreading to small intrahepatic vessels and bile ducts because of high pressure gradients that occur during ablation.28 These could be the main cause of high rate of recurrence in the initial first year post treatment. In our study, the cumulative rate of tumor recurrence in the first year was much higher than that following NAHR.
Tanaka et al.29 compared the survival impact of anatomic versus non anatomic resection in patients with solitary HCC. The 1, 3, and 5-year disease-free survival rates in the non-anatomic group were 21%, 52%, and 76% respectively. The 1, 3, and 5-year OS rates in the non-anatomic group were 97%, 91%, and 61% respectively. Okamura et al.30 compared the disease-free survival and OS rates using propensity matching analysis in the non-anatomic resection group and found that the cumulative 1, 3 and 5-year recurrence-free survival rates were 69.7, 46.5 and 31.9% respectively, and the cumulative 1, 3, and 5-year OS rates were 96.4%, 90.1% and 79.7% respectively. Wang et al.17 compared overall survival and disease-free survival between surgical resection and RFA. They found that for patients who underwent RFA the 1, 3, and 5-year cumulative OS rates were 98.1%, 82.8, and 82.8% respectively, and the 1, 3, and 5-year cumulative disease-free survival rates were 67.1%, 46.4%, and 38.0%. Our study found similar results of recurrence and OS rates.
Goh et al.31 reported that the number of tumors (>3 nodules) was an independent negative predictor of disease-free survival and OS. Increasing number of tumors means multiplicity of liver fibrosis, as liver fibrosis increase the risk of carcinogenesis. Tumors recurred simultaneously at remnant liver tissue, even though hepatic resection or RFA were carried out. In this study, we performed univariate analysis and multivariate cox proportional hazard regression analysis. Only tumor number affected recurrence rate in the multivariate analysis.
As aforementioned, liver function is related to liver fibrosis, and liver fibrosis is associated with carcinogenesis of the liver. In this study, albumin, number of tumors, and MELD score, statistically affected recurrence rate, whilst Albumin and INR statistically affected OS rate in univariate analysis. The other liver function related factors tested were not related to recurrence and OS rates with statistical significance. We think this is most likely due to small sample size, and short-term follow-up study. Although, without statistically significant differences, liver function-related factors, including PT INR, albumin, total bilirubin, and grading systems (Child-Pugh class and MELD score) also seems to be a prognostic factor of overall survival rate and recurrence rate. This suggests that the severity of the underlying liver disease may be a risk factor of HCC recurrence and overall survival. It also supports the importance of liver status in carcinogenesis.
HCC patients with low levels of AFP and PIVKA-II had more favorable clinical characteristics and showed a better prognosis than those with elevated levels of AFP or PIVKA-II.32 We found that tumor markers were not related to tumor recurrence or OS. We attempted to evaluate the tumor markers for each patient before operation, but some patients were missing. Additionally, we checked PIVKA-II for preoperative patients but could only gather a small data set.
Our study had several limitations. First of all, our study included a small sample size and short follow-up period. We think that this accounts for the absence of statistically significant differences. Secondly, it was a retrospective study. Thus, our study has fundamental flaws by a selection bias. We overcame selection bias by using propensity score matching methods, but it made a result from a smaller sample size.
In this study, the tumor number is a predictor of disease free survival and albumin is a predictor of overall survival in small sized HCC patients. We recommend non-anatomical hepatic resection over intraoperative RFA in small sized HCC, because of high recurrence rate in intraoperative RFA. We did not find intraoperative RFA to be inferior to NAHR in any other way, except recurrence rate. Clinicians need to select the optimal treatment considering liver function and possibility of recurrence. Our study highlights the requirement for a large volume long-term follow-up study to further analyze these treatments and when they are best applied.

 XML Download
XML Download