

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Central nervous system (CNS) affection taking the form of supratentorial, cerebellar, or spinal cord abscesses from hematogenic dissemination of a pulmonary infection with Nocardia sp. is a rare finding,1,2 and the induction of nocardiosis due to long-term therapy with corticosteroids for idiopathic thrombocytopenia (ITP) is more rarely found.3-5 Two of these cases developed supratentorial abscesses. However, both cerebellar and supratentorial abscesses from Nocardia sp. in a patient under corticosteroids for ITP, have not been reported.
CASE REPORT
The patient is an 83 years-old, human immunodeficiency virus (HIV)-negative, Caucasian male, with a history of recurrent nasal bleedings since childhood, recurrent gingival bleedings, frequent cutaneous hematoma after minor traumata, which were attributed to ITP diagnosed at age 52 years, splenectomy at age 52 years for the ITP, coronary heart disease resulting in two myocardial infarctions at age 52 years, corticosteroids for ITP since age 53 years, steroid-induced diabetes mellitus since age 53 years, requiring insulin since age 78 years, arterial hypertension since years, hyperlipidemia since age 53 years, percutaneous transluminal coronary angioplasty at age 62 years, aortocoronary bypass grafting at ages 64 and 75 years, atrial fibrillation since age 68 years, cataract surgery at ages 71 and 74 years, bilateral carotid artery stenosis requiring stent implantation at age 72 years, a 6-fold stent placing for coronary stenoses at age 75 years, bilateral hypoacusis since age 78 years requiring hearing devices bilaterally and sensori-motor polyneuropathy since age 78 years. Since age 82 years, he also noted a mild cognitive decline and non-specific visual impairment and started to use a stick for walking and a walker since two weeks prior to admission. His family history was positive for diabetes mellitus and short stature in his mother. From age 68 years until admission, he was taking phenprocoumon.
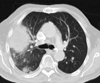
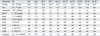
He was admitted at age 83 years because of chronic tiredness, dyspnea, hemoptysis, and abdominal pain. Blood chemical findings showed leucocytosis with a maximum value of 38.8/nL (n, 4.0-9.0/nL) on hospital day (hd) 3, thrombocytopenia with a minimum value of 4/nL (n, 150-450/nL) on hd 15 and hd 18, renal insufficiency, and elevated C-reactive protein with a maximum value of 34.7 mg/dL (n, ≤ 0.6 mg/dL) at hd 3 (Table 1). There were also elevated glutamate-oxalate transaminase, glutamate pyruvate transaminase, and lactate dehydrogenase (Table 1). Creatine-kinase was normal throughout hospitalization. There was slight hypocalcemia (Table 1) and elevation of ferritin to 3817 ng/mL (n, 30-400 ng/mL). Thyroid function parameters were indicative of hyperthyroidism. The HbA1c was 7.4% (n, ≤ 6%). X-ray of the lung revealed multiple reticulonodular infiltrates up to one cm in diameter over both lungs with predominance in the left lower lobe, a pleural effusion in the horizontal interlobar fissure, and an encapsulated effusion in the right-sided diagonal interlobar fissure. X-ray of the lung five weeks earlier had been normal. A CT-scan of the thorax showed an 11×7 cm, enhancing mass lesion in the right upper lobe with central and peripheral necrosis and multiple irregularly contoured hyperdensities over both lungs (Fig. 1). Sputum cultures grew Nocardia sp.
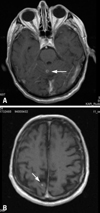
Clinical neurologic examination revealed slight dysarthria, dysphagia, bilateral ptosis, bilateral hypoacusis, postural tremor, left-sided dysdiadochokinesia, weakness for hip extension bilaterally (M5-), reduced tendon reflexes on the upper limbs and absent tendon reflexes on the lower limbs, diffuse wasting, stocking-type sensory disturbances bilaterally, and ataxic stance. He was able to walk with a walker. MRI of the cerebrum showed a hyperintense, enhancing lesion of 4 mm in diameter in the cranial part of the cerebellar vermis (Fig. 2). Additionally, there were small hyperintense lesions in the occipital deep white matter and subcortically bilaterally (Fig. 2). Lumbar puncture was recommended, but contraindicated due to ITP. No manifestations of nocardiosis other than in the lung and cerebrum were detected.
For ITP, the patient received prednisolone 50 mg/d until hd 9. For the general infection, he initially received amoxicillin between hd 2 and hd 4. From hd 4 to hd 7, he received caspofungin and between hd 5 and hd 7 piperazillin. Meropenem was started on hd 8 and maintained until hd 45. He had never developed fever during the entire hospitalization. After dismissal, the patient was switched to a long-term therapy with trimethoprim-sulfamethoxazol. Shortly after admission, oral anticoagulation was stopped because of severe thrombocytopenia of 4,000/nL (Table 1). Since hd 23, corticosteroids had to be restarted because of deteriorating ITP (Table 1). His therapy at dismissal included danazol, furosemide, pantoprazole, atorvastatin, metoprolol, enalapril, amiodarone, prednisolone, folic acid, and insulin in addition to the antibiotic. At the three month follow-up, dimension of the pulmonary lesions had regressed. On the contrary, the cerebral lesions had progressed despite trimethoprim-sulfamethoxazol, promting a switch to sultamicillin and then to meropenem. Unexpectedly, the patient died from acute myocardial infarction shortly thereafter. Autopsy excluded a pulmonary malignancy as the underlying cause of nocardiosis and confirmed that antibiotic therapy was not effective in eradicating the cerebral infection, although cerebral tissue cultures were negative for Nocardia sp.
DISCUSSION
Nocardiosis is an opportunistic local infection with consecutive hematogenic spread in half of the cases from the Gram-positive, filamentous, eosinophilic organism Nocardia sp. The most frequently found species is N. farcinica,6,7 followed by N. asteroides,8-10 N. paucivorans,11 N. otitidiscaviarum,12 N. brasiliensis,13 N. cyriacigeorgica,14,15 or N. transvalensis.14,16,17 Nocardiosis is an uncommon disease, but its frequency has increased due to the high number of immunosuppressive treatments, improved diagnostic facilities, and increasing survival times of patients with malignancy.18 Patients become infected by inhalation, direct traumatic cutaneous inoculation, or by eating contaminated food.19 The most common primary site of nocardiosis is the respiratory tract, being the origin of hematogenic dissemination with a high incidence to the skin, subcutaneous tissue, or CNS.6,19,20 Extra-pulmonary manifestations of nocardiosis include CNS abscesses or meningitis,6 chorioiditis,6 intraocular vasculitis,21 or renal abscesses.22 Most patients have an underlying chronic diseases or suffer from endogenous or drug-induced immunosuppression with for instance TNF-alpha blockers, but Nocardia can also infect healthy subjects.23 Culture or biopsy followed by identification of the infectious species by PCR is recommended because of the specific therapeutic strategies associated with each species and their different sensitivity to antibiotics.6 Because of the high relapse rates, treatment is recommended to be continued for 12 months.24
CNS nocardiosis usually manifests as cerebral abscesses or rarely as meningitis or chorioiditis. The abscesses usually develop supratentorially but cerebellar abscesses have been also reported (Table 2).2,25-27 Though the preference of Nocardia sp. for the CNS is well known, CNS abscesses from Nocardia sp. are rare and account for only 1-2% of brain abscesses.1,28 In almost half of the patients with pulmonary nocardiosis, dissemination is associated with brain abscesses.10 Early detection and treatment is important because the mortality is three times higher than that of other bacterial cerebral abscesses.28 Since the literature about CNS nocardiosis takes the form of anecdotal reports, small case series, or retrospective studies (Table 2), an optimal treatment approach has not yet been established. Abscesses with Nocardia sp. represent a diagnostic and therapeutic challenge, since they are associated with high mortality rates, particularly in immunocompromised patients. Cerebral abscesses are managed either conservatively with stereotactic aspiration, or by open craniotomy and enucleation.29 Surgical treatment is indicated if the lesions are large and readily accessible or in case of progression of the lesions within two weeks after initiation of the antibiotic treatment. There is growing evidence that the size of the cerebral lesion and clinical and immune status of the patient are relevant to surgical decision making. In spite of the existing controversy with regard to the surgical management of these lesions, an early diagnosis through stereotactic aspiration and the beginning of an antibiotic therapy are essential for a favorable outcome.19 In most cases of cerebral nocardiosis the overall prognosis is favorable upon adequate antibiotic or surgical therapy.30 However, there are several cases with poor outcome (Table 2).18,25,31
The patient presented herein is interesting because of severe side-effects to long-term corticosteroid treatment for ITP, including pulmonary and cerebral nocardiosis, induction of diabetes shortly after initiating corticosteroids at age 53 years, cataract, and possibly steroid myopathy. Whether corticosteroids could be responsible also for arterial hypertension, dermal atrophy, or dermal bleedings remains speculative. Since arterial hypertension had occurred already prior to the administration of steroids, a causal relationship is rather unlikely. It also remains elusive if myopathy was due to the side-effects of corticosteroids alone or due to other causes. The combination of thrombocytopenia, diabetes, and hypoacusis has been reported together with the thiamine-responsive megaloblastic anemia syndrome,32 but anemia was not a dominant feature in the present patient. The combination of diabetes, hyperlipidemia, arterial hypertension, atrial fibrillation, thrombocytopenia, sensorineural hearing loss, the renal cyst, myopathy, and cataract could also be attributed to a systemic metabolic defect as the underlying pathology. Unfortunately, however, further diagnostic work-up into this direction was limited due to the ITP. The cause of the markedly elevated ferritin levels remains elusive, but could be explained with the chronic infection. Pulmonary malignancy was definitively excluded at autopsy. The slightly reduced calcium levels were attributed to hypoalbuminemia. That the antibiotic therapy definitively eradicated the infection with Nocardia sp. remains speculative since negative culture results cannot be reliably interpreted as evidence that the infection was eradicated. Whether the patient was resistent to the applied antibiotics and would have profited from linezolid, as has recently been reported,33 is unknown.
The present case shows that long-term therapy with corticosteroids for ITP may induce immune-incompetence, resulting in the development of pulmonary and cerebral nocardiosis. Cerebral nocardiosis may not sufficiently respond to long-term antibiotic therapy and may necessitate switching to alternative antibiotics or surgery. Long-term corticosteroid therapy may induce secondary steroid myopathy or enhance primary metabolic myopathy.

 XML Download
XML Download