

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The development of bilateral ureteral obstruction after appendectomy is an uncommon but well recognized complication of appendicitis.1-3 The condition is usually caused by complications associated with appendicitis or with the surgical sequelae of appendectomy. Here, we report the development of anuria after appendectomy in a patient with a single kidney containing a distal ureteral stone. We also discuss the importance of radiological evaluation in the differential diagnosis of acute appendicitis and the possible causes of anuria after appendectomy.
CASE REPORT
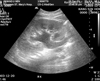
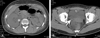
A 20-year-old woman was transferred to our hospital due to a sudden cessation of urine output after appendectomy. She had been well until the day of the operation. On that day, the patient experienced nausea and vomiting in the morning, and pain in the epigastric area had migrated to the right lower quadrant by the afternoon. At a local clinic, she was a diagnosed with appendicitis and an exploratory laparotomy was performed. Just after surgery, there was a sudden cessation of urine output, and she was transferred to our hospital. In the emergency room, her vital signs were stable. A physical examination revealed a mildly dry tongue and mild tenderness at the operation site. Laboratory studies were remarkable for a white blood cell count of 14.98 × 109/L and a serum creatinine level of 265.2 µmol/L. Urinalysis revealed microscopic hematuria (20-30 red blood cells per high-power field). A chest radiograph showed no evidence of pulmonary edema or cardiomegaly. An additional radiological evaluation with abdominal sonography revealed a hydroureter in her single right kidney (Fig. 1). A non-enhanced abdominal computed tomography (CT) scan revealed a calcified stone at vesicoureteral junction in the kidney (Fig. 2A, B). A foley catheter was inserted, but the urine output remained scanty. Hydration using intravenous normal saline and furosemide (40mg) treatment was performed, and the urine output increased gradually by 4 h. Serum creatinine levels decreased from 265.2 µmol/L to 149.4 µmol/L. On the patient's second day in hospital, a double-J catheter was inserted using cystoscopy examination. Excretory intravenous pyelography revealed a persistent hydroureter and distal ureteric stricture (Fig. 3), and the serum creatinine level normalized (78.7 µmol/L).
DISCUSSION
The development of acute renal failure after appendectomy is usually related to either a ureteral injury caused during appendectomy or a complication of appendicitis, such as pelvic inflammation,1 appendiceal abscess2 or trigonal edema.3 In this patient, we initially considered a surgical complication as the cause of acute renal failure because the urine output decreased so abruptly after surgery. However, a retrospective review of the patient's medical records at the local clinic showed an elevated serum creatinine level (291.7 µmol/L) at the time of admission. This suggested that her renal dysfunction was not related to a surgical complication during appendectomy. Radiologic evaluation with abdominal sonography and CT scans revealed that the cause of anuria after appendectomy was related to obstructive nephropathy caused by a distal ureteral stone in her single kidney. This case indicates the importance of radiological evaluation before appendectomy and the importance of differential diagnosis of acute renal failure following appendectomy.
Because the complete absence of one kidney is clinically silent, the diagnosis usually is not suspected; the condition typically remains undetected unless careful examination of the external and internal genitalia reveals an abnormality that is associated with renal agenesis, or unless an imaging study done for other reasons reveals only one kidney.4 If the patient had possessed two kidneys, anuria may not have occurred after appendectomy because the contralateral kidney would have been able to excrete urine. Thus, the diagnosis of a distal ureteral stone might have been delayed until she experienced further renal problems. Moreover, a diagnosis of obstructive nephropathy may be missed in such patients since distal ureteral stones often pass out spontaneously. Thus, it was the development of anuria in this patient that enabled us to diagnose this congenital anomaly.
Ureteral anomalies are frequently observed in patients with the complete absence of one kidney. In general, the ipsilateral ureter is completely absent or partially developed. Partial ureteral development is associated with complete luminal atresia or patency to variable degrees.5 In this patient, it is uncertain whether distal ureteral stricture was related to the developmental anomaly or if it was secondary to stone formation. However, in general, we suggest radiological evaluation of the distal ureter in patients with congenital renal agenesis due to the high incidence of ureteral anomalies in such patients.
The diagnosis of acute appendicitis is usually made from clinical manifestations and laboratory findings, but the importance of radiological evaluation is increasing because there is a high incidence of negative appendectomy. The introduction of abdominal CT scans has decreased the incidence of negative appendectomy from 17% to 2%.6 In this case, radiological evaluation was not initially performed because the clinical manifestations and laboratory findings were compatible with acute appendicitis. However, if a radiological evaluation was performed, the patient's obstructive nephropathy could have been diagnosed before the appendectomy, and anuria after appendectomy could have been prevented. Although it remains controversial whether radiological evaluations should be done for all patients with suspected appendicitis, we recommend it for the prevention of unexpected events that were observed in this patient.
We report the simultaneous presentation of acute appendicitis and a distal ureteral stone in a patient with a single kidney. Based on this case, radiological evaluation is strongly recommended in patients with suspected acute appendicitis.

 XML Download
XML Download