

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Advanced malignant tumors of the hepatic hilum are difficult to treat, both surgically and nonsurgically (1). Transhepatic or endoscopic placement of a metallic stent is a well-established palliative treatment for an advanced hilar malignancy (2, 3, 4, 5, 6, 7, 8).
There have been conflicting opinions regarding whether unilateral or bilateral stents should be placed (4, 8, 9, 10, 11, 12, 13). Some clinical investigators prefer bilateral stenting, not only because unilateral stenting alone may not completely relieve jaundice (10) and may induce acute cholangitis (11), but also because stent patency may be longer than with unilateral stenting (8). However, other authors advocate unilateral drainage because the complication risk is lower than when deploying several stents (13) and because adequate palliation can be achieved by draining only 25% of the liver (9). Previous studies (1, 14) have shown that placing a unilateral biliary metallic stent in the liver lobe with a patent portal vein is a safe and effective palliative treatment for patients with a contralateral portal vein occlusion caused by advanced hilar malignancy; thus, obviating the need for placing bilateral stent in these patients.
We investigated the safety and efficacy of percutaneous unilateral metallic stenting using covered and uncovered stents in 60 patients with a malignant biliary hilar obstruction and a contralateral portal vein steno-occlusion.
MATERIALS AND METHODS
Patient Population
Sixty consecutive patients (31 men and 29 women; mean age, 64 years; range, 36-81 years) with a malignant hilar biliary obstruction and contralateral portal vein steno-occlusion, i.e., severe stenosis (> 90% luminal narrowing on computed tomography [CT]) or complete occlusion (encasement of the portal vein with no demonstrable flow or an intraluminal filling defect), caused by tumor invasion or pre-operative embolization for resection from October 2010 to October 2013, were treated by percutaneous placement of biliary metallic stents. Thirty-nine of these patients had a portal vein occlusion. Twelve had severe portal vein stenosis caused by underlying malignant tumors, whereas nine had a portal vein occlusion caused by preoperative portal vein embolization using vascular plugs, coils, or Gelfoam particles. A curative surgical treatment could not be performed in these nine patients due to major vessel invasion or peritoneal seeding. Demographic, clinical, and laboratory data were collected from the medical records of all patients or from the electronic patient information database. Accurate and definitive follow-up data were obtained for all 60 patients. This retrospective study was approved by our Institutional Review Board, and the requirement for written, informed consent from each patient was waived.
The patient characteristics are presented in Table 1. The diagnosis was confirmed histopathologically in 46 patients (77%) through a percutaneous transbiliary forceps biopsy in 25 patients and by endoscopic brush cytology and forceps biopsy in 21 patients. The diagnoses were presumed in the other 14 patients (23%) based on CT and magnetic resonance cholangiopancreatography results. Patients were included if they had a malignant biliary hilar obstruction and a unilobar portal vein steno-occlusion or embolization that could not be treated surgically due to unresectability, late tumor stage, advanced age, co-morbidities, or if endoscopic attempts to drain obstructed bile ducts were unsuccessful. Exclusion criteria included abnormal coagulation status (international normalized ratio value ≥ 1.5), platelet count ≤ 50000, or a generally poor health status (Eastern Cooperative Oncology Group performance status grade 3-4).
Technique
Computed tomography or magnetic resonance cholangiography was performed to access patient anatomy and determine the most appropriate interventional approach before percutaneous transhepatic biliary drainage (PTBD). All PTBD procedures were performed in the peripheral bile duct, and the patients were under conscious sedation with intravenous pethidine hydrochloride (Demerol; Keukdong, Seoul, Korea) and with local anesthesia using intramuscularly injected lidocaine (Jeil, Daegu, Korea) at the PTBD site. The intrahepatic bile duct was punctured using a 21-gauge Chiba needle (Cook Medical, Bloomington, IN, USA) under fluoroscopic guidance or ultrasonography, and a 8.5-Fr drainage catheter was inserted to relieve jaundice or cholangitis before inserting the stent. Stents were placed for less than 2 weeks after PTBD; thus, allowing any cholangitis to be treated. Antibiotics were administered intravenously 2 hours before the procedures and for at least 48 hours after. Intravenous antibiotic therapy was maintained in patients with cholangitis until the treatment was successful.
The stent insertion procedure was as follows. A 5-Fr Kumpe catheter (Cook Medical) and a 0.035-inch guidewire (Radifocus Guide Wire M; Terumo, Tokyo, Japan) were advanced across the hilar obstruction to the common bile duct or duodenum. Balloon dilation was performed in all patients before placing the stent using a 6-8-mm-diameter angioplasty balloon catheter (Synergy; Boston Scientific, Galway, Ireland).
All stents deployed were uncovered (Zilver [Cook Medical], Sentinol stents [Boston Scientific]), partially expanded polytetrafluoroethylene (ePTFE)-covered (Hercules [S&G Biotech, Seongnam, Korea], Comvi [TaeWoong Medical, Gimpo, Korea], or GD stents [TaeWoong Medical]). The Zilver and Sentinol stents were made of nitinol with laser cutting and have high flexibility and minimal foreshortening during deployment. All covered stents were partially ePTFE-covered nitinol stents. The partially ePTFE-covered stents had bare extensions of 2 or 3 cm at the proximal end to prevent tumor overgrowth, migration, and intrahepatic bile duct occlusion. All stents were available in 8 and 10 mm diameters and in 6 and 8 cm lengths. The type, diameter, and length of each stent were decided by physician's preference.
Our stent deployment system was introduced over a 0.035-inch, 150-cm long stiff hydrophilic guidewire (Terumo) or over an extra-stiff Amplatz guidewire (Cook Medical) and was deployed across the hilar obstruction to the common bile duct to cover the bile duct approximately 1-2 cm proximal and 2-3 cm distal to the obstruction to prevent tumor overgrowth. Post-stenting balloon dilation was not performed in any patient. After the procedure, an 8.5-Fr or 10-Fr temporary drainage catheter (Cook Medical) was placed just proximal to the stent. The external drainage catheter was irrigated frequently for 1-2 days after placement to remove any possible blood clots or sludge. The temporary drainage catheter was removed after 2-3 days of catheter clamping, and without further intervention if free contrast flowed through the stent into the common bile duct and the duodenum. Information regarding the current health status or death of patients was obtained by telephone or from their medical records.
Study Endpoints and Definitions
The study endpoints were the rates of technical success, complications, successful internal drainage, stent patency, and patient survival time. Technical success was defined as stent deployment in an appropriate position across the stricture with good contrast passage through the stent. Complications were classified as major and minor according to the guidelines of the Society of Interventional Radiology Standards of Practice Committee (15). Successful internal drainage was defined as successful removal of the temporary drainage catheter and a decrease in serum bilirubin level to < 75% of the pretreatment value within the first month following placement of the stent. Patient survival time was defined as the time interval between initial stent placement and death. Stent patency was defined as the period between initial stent placement and recurrence of the obstruction or death with a patent stent. A stent was assumed to be patent at the time of death if serial serum bilirubin levels were normal or only mildly elevated (< 3 mg/dL). Stent occlusion was defined as a radiologically confirmed biliary obstruction with a serum bilirubin level > 3 mg/dL or as any condition requiring a repeat intervention to improve biliary drainage. Sludge formation was defined as sludge occluding the stent lumen and that could be cleared by a biliary balloon sweep. Tumor ingrowth was defined as tissue occluding the stent lumen and that could not be cleared by a biliary balloon sweep. Tumor overgrowth was defined as a new stricture occurring at the proximal or distal end of a stent.
Statistical Analysis
All statistical analyses were conducted using SPSS ver. 14.0 software (SPSS Inc., Chicago, IL, USA) A p value < 0.05 was considered statistically significant. The paired-sample t test was used to compare serum bilirubin levels before and after stent placement. Patient survival time and stent patency were estimated using a life-table analysis, according to the Kaplan-Meier method. The comparison of stent patency between covered and uncovered metallic stents was conducted using the log-rank test.
RESULTS
Procedural Outcomes and Complications
Stents were successfully placed in all 60 patients. Control cholangiography performed immediately following stent placement confirmed correct positioning of all stents. None of the covered stents migrated after deployment. The 60 patients received a total of 70 stents. A single stent was sufficient to relieve the malignant hilar obstruction in 51 patients (Fig. 1), whereas two stents were placed in the ipsilateral bile ducts of the remaining nine patients with multiple separation of the ipsilateral, intrahepatic bile duct (Fig. 2). Twenty-seven patients received 33 covered stents, and 33 patients received 37 uncovered stents of different sizes.
Procedural-related minor complications occurred in six (10%) patients. Two patients experienced self-limiting hemobilia that resolved completely without a transfusion 1-3 days following stent placement. Cholangitis occurred in four patients, two of whom underwent placement of a covered stent and two who underwent placement of an uncovered stent. However, all four patients with cholangitis showed favorable clinical courses within 4 days following antibiotic treatment and without the need for additional intervention. Two patients developed acute cholecystitis 11 and 350 days, retrospectively, following placement of a biliary stent and underwent percutaneous gallbladder drainage.
The follow-up cholangiography performed 3-6 days after placing the stents showed adequate decompression of the biliary ducts in 54 patients. The temporary drainage catheters were removed in these 54 patients after confirming good passage of contrast medium through the stent. The temporary drainage catheters could not be removed in six patients who underwent placement of uncovered (n = 3) and covered (n = 3) stents due to persistently high serum bilirubin levels (n = 5) or stent dysfunction (n = 1). One patient had an uncovered stent dysfunction caused by early tumor ingrowth; however, the temporary drainage catheter could not be removed due to the patient's refusal to undergo additional stent placement. Mean serum bilirubin level, which was 10.35 ± 8.0 mg/dL before drainage, decreased significantly to 1.96 ± 2.3 mg/dL 1 month after placing the stent (p < 0.001). Successful internal drainage was achieved in 54 (90%) of the 60 patients.
Patient Survival
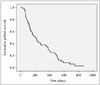
All patients were clinically followed until their death or until the end of the study, and the cutoff date for data analysis was December 31, 2013. During the mean follow-up period of 268 days (range, 27-862 days), 55 patients died, and five patients survived. One patient died within 30 days after placement of a stent due to rapid progression of underlying malignancies; death was not directly related to the procedure. According to the Kaplan-Meier analysis, the median survival time was 210 days (95% confidence interval [CI], 135-284 days) (Fig. 3).
Stent Patency
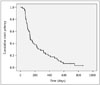
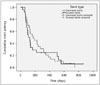
According to the Kaplan-Meier analysis, median stent patency time was 133 days (95% CI, 94-171 days), and the cumulative stent patency rates at 1, 3, 6, 9, and 12 months were 100%, 97%, 46%, 28%, and 21%, respectively (Fig. 4). No significant difference in stent patency was observed between covered and uncovered stents (p = 0.646) (Fig. 5). Stent dysfunction occurred in 16 (29.6%) of 54 patients after a mean of 159 days (range, 65-321 days). Stent dysfunction caused by tumor ingrowth occurred in all 10 patients who received an uncovered stent, whereas stent dysfunction caused by sludge incrustation (n = 5) or tumor overgrowth (n = 1) occurred in only six patients who received a covered stent (Table 2). Stent dysfunctions were managed using the PTBD procedure in 16 patients. Four patients with a stent dysfunction caused by tumor ingrowth (n = 3) or sludge incrustation (n = 1) received another covered stent, resulting in good internal drainage before these patients died. An additional metallic stent was not placed due to disease progression and poor general health in the remaining 12 patients.
DISCUSSION
In general, the most important factor regulating the volume of bile flowing is the rate of bile salt synthesis by hepatocytes, which is regulated by the return of bile salts to the liver through the enterohepatic circulation. A portal vein obstruction interrupts the enterohepatic circulation cycle in the obstructed lobe (1, 16). Previous investigators have reported successful treatment of bile leakage by selective portal vein embolization, which stops bile production (17, 18). Thus, a liver lobe with a portal vein occlusion caused by an advanced hilar malignancy stops producing bile and becomes nonfunctional and atrophied. Hepatic lobar atrophy is also frequently accompanied by hilar cholangiocarcinoma, which occurs in 20-30% of patients with this diagnosis (19, 20, 21). Hadjis et al. (19) reported that biliary decompression of the lobe with a portal vein occlusion does not reverse the atrophy or improve liver function. Other authors (20, 21) have recommended that biliary drainage should be performed in the non-atrophic lobe. Based on these results, we postulated that unilateral stenting in a lobe with a patent portal vein may be preferable in patients with a contralateral portal vein occlusion caused by an advanced hilar malignancy or portal vein embolization, as bile production in the undrained lobe may be functionally impaired or prevented by the portal vein occlusion.
We achieved a 100% technical success rate, 10% complication rate (10%), 90% successful internal drainage rate, and a 210 day median patient survival time, which are in good agreement with other similar studies (2, 3, 4, 5, 6, 7, 8, 10, 13, 14, 22, 23, 24, 25). In those studies, technical success rates were 93-100%, overall complication rates were 17-33%, successful internal drainage rates were 89-92%, and median patient survival time was 176-239 days. We also found a median stent patency time of 133 days (95% CI, 94-171 days), and the cumulative stent patency rates at 1, 3, 6, 9, and 12 months were 100%, 97%, 46%, 28%, and 21%, respectively. Two previous studies using uncovered or covered stents showed that placing a unilateral stent in the lobe with the patent portal vein is a feasible, safe, and effective method for palliative treatment of patients with contralateral, portal vein occlusion (1, 14). However, we used both covered and uncovered metallic stents.
Covered stents were initially developed for the biliary system to address tumor ingrowth. Use of a PTFE-covered stent is effective, as the PTFE is an effective barrier to prevent tumor ingrowth (14). In one comparative study of ePTFE-covered and uncovered stents (26), ePTFE-covered stents were significantly superior to uncovered stents in terms of stent patency. It is difficult to compare our results with those of other comparative studies because patients have different types, locations, and stages of disease; however, we found no significant difference in stent patency between ePTFE-covered and uncovered stents. Although a covered stent effectively prevented stent dysfunction caused by tumor ingrowth, covered stents stopped functioning mainly due to sludge incrustation. Further investigations will be required to determine how to decrease sludge formation.
Our study had limitations, including its retrospective nature. Moreover, further prospective, randomized comparisons are necessary, as differences among the five stent types we used may have influenced the stent patency result.
In conclusion, unilateral placement of ePTFE-covered and uncovered stents in the lobe with a patent portal vein is a safe and effective method for the palliative treatment of patients with contralateral portal vein steno-occlusion caused by advanced hilar malignancies or portal vein embolization. No difference in stent patency was observed between ePTFE-covered and uncovered stents in these patients.




 XML Download
XML Download