

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Since Alexander Duane published a paper in 1905 describing what has come to be known as Duane's retraction syndrome, Thomas Duane reported a similar, yet different set of symptoms and signs as 'pseudo-Duane's retraction syndrome' in 1976.1 In the most common type of Duane's retraction syndrome, there is markedly restricted abduction with eyeball retraction and narrowing of the palpebral fissure on adduction.2 In pseudo-Duane's retraction syndrome, however, abduction of the affected eye is possible to some extent, and the globe retraction occurs on abduction accompanied by narrowing of the palpebral fissure presenting the opposite features as those of classic Duane's retraction syndrome. The etiology is also completely different from those of Duane's retraction syndrome. Pseudo-Duane's retraction syndrome has been reported as being caused by acquired or congenital factors that affect the medial rectus muscle. Entrapment of the medial rectus muscle in a medial orbital wall fracture has been known to be the most common cause.3
We report a case of pseudo-Duane's retraction syndrome with entrapment of the medial rectus muscle in an old medial orbital wall fracture, presenting very similar clinical features as those of classic Duane's retraction syndrome. The presentation is contradictory to previous reports of pseudo-Duane's retraction syndrome.
Case Report
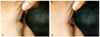
A 15-year-old boy had complained of motility limitation in the right eye since a young age. His visual acuity was 20/20 in each eye, although an ocular motility examination revealed markedly limited abduction and mildly limited adduction in his right eye (Fig. 1). On attempted adduction of the right eye, globe retraction (Fig. 2) with narrowing of the palpebral fissure was observed, and there mild upshoot and downshoot were also observed (Fig. 1). The palpebral fissure of the right eye was slightly widened on attempted abduction. An alternate prism cover test revealed a 16 prism diopters (PD) right esotropia (ET) in the primary position, 25 PD ET in right gaze, 10 PD ET in left gaze at distance fixation, and 4 PD ET at near fixation. He assumed a compensatory face turn to the right and did not complain of diplopia. No living member on either the paternal or maternal side had a squint. Duane's retraction syndrome was inferred as the diagnosis until we noted that the patient's right eye had slight enophthalmos. Hertel's exophthalmometry revealed a 1.5 mm difference between both eyes and the margin reflex distance 1 was 0.5 mm in the right eye. Computed tomography of the orbits was performed and demonstrated an old medial orbital wall fracture with entrapment of the medial rectus muscle and surrounding tissues (Fig. 3). However, there was no history of trauma or forceps delivery according to the patient or his parents. A forced duction test under topical anesthesia was definitely positive in the right eye. The patient's ocular motor impairment was concluded to have arose from a long-term medial orbital wall fracture and was diagnosed as 'pseudo-Duane's retraction syndrome'. Because open reduction surgery for an old orbital wall fracture would be very difficult, and fruitless for this patient, we decided only to perform surgery on the eye muscle. The 5 mm recession of the right medial rectus muscle was successfully performed in order to correct the patient's head turn and esotropia. Neither structural anomalies nor fibrosis of the medial rectus muscle was observed during surgery. Postoperatively, the patient had orthotropia in the primary position, and the anomalous head posture disappeared, though there were still some limitations in both abduction and adduction in the right eye one year after the surgery.
Discussion
Duane's retraction syndrome is a well-known congenital ocular motility disorder caused by anomalous innervation and mechanics of the lateral rectus muscle, with secondary muscle changes sometimes superimposed. In 1976, Thomas Duane reported five cases of pseudo-Duane's retraction syndrome showing similar, yet different, symptoms and sign as Duane's retraction syndrome.1 Other authors preferred the names of 'inverse Duane, reverse Duane, or mirror-image Duane retraction syndrome' owing to the presentation of opposing clinical features compared with those of classic Duane's retraction syndrome. The etiology is, also, completely different from that of classic Duane's retraction syndrome. The primary lesion in pseudo-Duane's retraction syndrome is suspected to be the medial rectus muscle. Most cases have been reported to result from the entrapment of the medial rectus muscle within the medial orbital wall due to trauma.1,3 Congenital cases,4 recurrent pterygium,5 and myocysticercosis involving the medial rectus muscle6 have also been reported to be related with inverse Duane's retraction syndrome. In Korea, Jo et al.7 reported on inverse Duane's retraction syndrome with exotropia, and Lew et al.8 reported a case of congenital inverse Duane's retraction syndrome with a tight medial rectus muscle. Recently, a case of innervational etiology, such as bilateral inverse Duane's retraction syndrome, due to simultaneous co-contraction of both horizontal rectus muscles has been reported by Khan.9 To the best of our knowledge, there is no report presenting very similar clinical features as those of classic Duane's retraction syndrome arising from the entrapment of the medial rectus muscle in a medial orbital wall fracture. This case would most appropriately be categorized as pseudo-Duane's retraction syndrome instead of inverse or reverse Duane's retraction syndrome. There might be some possibility that the patient acquired Duane's retraction syndrome prenatally, and that the medial orbital wall then fractured after birth. However, several pictures of this patient around one year of age revealed that there was no conspicuous head turn, and his family recalled that the limited eye movement was not noted until 2-3 years of age. The limitation of his eye movements, therefore, could be concluded as acquired due to unnoticed orbital trauma after one year of age.
We report a case of pseudo-Duane's retraction syndrome caused by entrapment of the medial rectus muscle in an old medial orbital wall fracture presenting very similar clinical features as those of classic Duane's retraction syndrome. The importance of several tests such as the forced duction test and an imaging study should be emphasized in making the diagnosis for limited eye movement.


 XML Download
XML Download