

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The dominant subtype of prostate cancers are acinar type adenocarcinomas. Unusual subtypes of prostatic carcinomas account for about 5% to 10% of adenocarcinomas. Prostate ductal carcinoma is the most common subtype of prostatic cancer (1, 2). There is an association with acinar prostate carcinoma and ductal carcinoma occurs rarely in pure subtype (3).
Prostate ductal carcinomas are characterized by tall and pseudostratified epithelial cells. This is to the cuboidal epithelial cell layer found in prostate acinar carcinomas. Prostate ductal carcinoma shows a variety of architectural patterns (4). Gene expression research proposed that ductal and acinar prostate cancers have a similar gene expression level, with few discordant genes (5). For a recent report for the Gleason score, Epstein (6) suggested that these cancers should be graded as Gleason pattern 4, because ductal carcinoma showed similar behavior with Gleason 4+4 acinar prostate carcinoma. Pure prostate ductal carcinoma is seen in less than 1% of patients with prostate cancer, with mixed ductal carcinoma accounting for 5% of these patients. Prostate ductal adenocarcinoma is thought to have a higher Gleason score and stage at presentation (3, 7, 8).
Prostate ductal carcinoma can be seen in the peripheral zone or verumontanum, in association with prostate acinar carcinoma. Prostate ductal carcinoma is usually thought that is one of the manifestation of prostate acinar carcinoma in advanced stage, involving the location of periurethral ducts cancer cell, and therefore shows an aggressive pathological subtype (9, 10). When it is detected in biopsies, RP specimen generally shows adverse characteristics including a large percentage of tumor volume, high probability of extraprostatic extension, seminal vesicle invasion, positive surgical margins rate and lymph node metastasis, a high Gleason score (> 7) (8).
Prostate ductal carcinoma has also been considered to show more rapid progression after therapy and to be an independent predictor of disease specific mortality (11, 12). However this is unclear whether prostate ductal carcinomas shows more adverse prognosis when matched for PSA, Gleason score in biopy and clinical stage. We therefore evaluated the clinicopathological features and prognosis of prostate ductal carcinoma in comparison with prostate acinar carcinoma in our current study.
MATERIALS AND METHODS
Among 3,980 patients who took a radical prostatectomy (RP) and transurethral resection of the prostate (TURP), from 1999 to 2013 at our institution, the Asan Medical Center, 33 (2.5%) prostate ductal carcinomas were identified. From these 33 cases, we enrolled 29 patients in our current study who were diagnosed with prostate ductal carcinoma and underwent a radical prostatectomy. The excluded four cases comprised of one patient who had taken a TURP and three patients who had a lymph node metastasis. The percentage of prostate ductal carcinoma was evaluated by two urology-specialized pathologists and the pathology slides of our 29 patient study cohort were reviewed.
The most common pathological patterns of prostate ductal carcinoma identified were cribriform and papillary. As the high-grade prostatic intraepithelial neoplasia (HGPIN)-like prostate ductal carcinoma shows a favor characteristics, similar to a Gleason score of 3, these were excluded from further analysis on this basis. The cribriform of prostate ductal carcinoma is made by intraglandular epithelial gland connection which result in the formation of slit-like lumens. This differs from the acinar carcinoma cribriform, which is consisted of a round lumina and a cuboidal epithelium. The papillary formation usually mixed with cribriform patterns. The distinctive characteristics of intraductal prostate carcinoma and ductal carcinoma is a columnar epithelium which consisted of tall pseudostratified with an amphophilic cytoplasm, usually showed in cribriform patterns with slit-like lumens and true papillary formation. On the other hand, intraductal carcinomas have micropapillary tufts without fibrovascular cores and cuboidal cells and cribriform formation. Additionally, there is no basal cells in prostate ductal carcinomas, although there can be partial retention of basal cells as prostate ductal carcinoma locates within prostatic ducts (13).
The clinical characteristics of our study group, including demographics, pathological features, surgical methods, prostate specific antigen (PSA) level, and follow-up duration were obtained through a review of medical information. The control group (n=116) was selected among the 3,980 patients in the originally screened cohort. These control patients were matched to the prostate ductal carcinoma patients by biopsy Gleason score, clinical stage, age, and pre-RP PSA. We then compared the two groups for positive surgical margin rate, pathologic T, N stage, post-surgery Gleason score, and biochemical recurrence rate. We defined a biochemical recurrence as a post-surgery PSA level >0.2 ng/mL. The mean (range) of the follow-up period in the case and control groups after the initial procedure was 23.8±20.6 months and 58±10.5 months, respectively.
We used the chi-square test for statistical comparisons of proportions and P values of <0.05 were recognized as statistical significance. Clinical progression, survival from the surgery to overall death and the combined endpoint of clinical progression for the restaged patients was evaluated using the Kaplan-Meier analysis. All statistical analyses were conducted by SPSS 15.0 software (SPSS, Inc, chicago, IL, USA).
RESULTS
The mean age of our group (n=29) was 67.33±5.9 yr old and the mean PSA in these patients before their RP was 14.7±14.2 ng/mL. The mean follow-up was 23.8±20.6 months after the initial procedure. Twenty two patients (75.8%) had T1 and T2 clinical stage, seven patients (24.1%) had T3 clinical stage (Table 1). In the final pathology analyses, 19 patients (65.5%) had a Gleason score ≥8, 16 patients (55.1%) had ≥T3 stage and 13 patients (44.8%) had a positive resection margin. Five patients had pure form ductal type whereas 24 patients had mixed type with acinar carcinoma. One patient with a pure form ductal carcinoma died from disease progression.
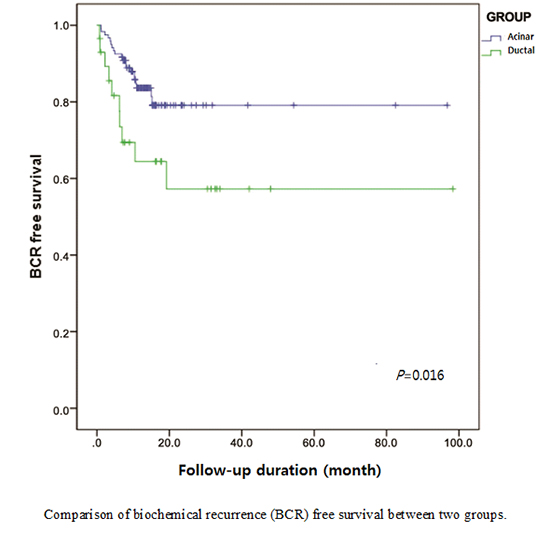
To further evaluate the clinicopathological features of our prostate ductal carcinoma patterns, we selected 116 patients as a control population from among the full cohort of 3,980 prostate acinar carcinoma patients treated at our institution. These control patients were matched to the ductal carcinoma patients by biopsy Gleason score, clinical stage, age, and PSA. The mean age of this control group (n=116) was 67.0±5.3 yr old and the mean PSA level before RP was 16.2±17.6 ng/mL. The mean follow-up duration in these control acinar carcinoma cases was 58±10.5 months after radical prostatectomy. When we compared our two study groups in terms of pathology stage, post surgery Gleason score and the positive resection margin rate, we found no statistically significant difference between any of these parameters other than the post surgery Gleason score which was ≥8 in ductal carcinoma (P=0.024) (Table 2). Additionally, we compared the biochemical recurrence rate in the two groups and biochemical recurrence-free survival duration. Ten patients (34.4%) showed biochemical recurrence in ductal carcinoma group, however, 20 patients (16.6%) showed biochemical recurrence in acinar carcinoma group. A Kaplan-Meier curve revealed a higher risk of biochemical recurrence rate in prostate ductal carcinoma (P=0.016) (Fig. 1).
DISCUSSION
The diagnosis of prostate ductal carcinoma is difficult for cases in which it is mixed with acinar carcinoma or when it is associated with HGPIN. Prostate intraductal carcinoma reflects infiltration of high grade acinar carcinoma in the intraductal extension (14, 15). We can find overlap between the cribriform and micropapillary patterns of HGPIN and the morphology of prostate ductal carcinoma (16). Although HGPIN can have micropapillary formation, it does not show the true papillary structures of prostate ductal carcinoma. Prostate ductal carcinoma has slit-like lumina and columnar nuclei, in contrast to round-oval nuclei of cribriform HGPIN. This is difficult for distinguish prostate ductal carcinoma from the intraductal carcinoma (14, 15).
The characteristics of ductal carcinoma has changed from its first description in 1967 (17). In that report, its characteristics was mentioned that prostate ductal carcinomas is able to infiltrate locally but will rarely metastasize and develop centrally in the urethra. Several studies presented a high likelihood of failure and a contradictory report with advanced disease at RP. However, these old reports were made before the use of serum PSA to screen for prostate cancer (18).
Patients with ductal carcinoma have been found to be more likely to have a clinical stage T3 or more aggressive prostate cancer, which confirmed previous studies of a greater rate of advanced cancer at the RP for patients with ductal carcinoma (19). Despite a high clinical stage at RP, patients with ductal carcinoma show a similar possibility of metastasis to the lymph nodes when it is compared with acinar carcinoma present. It can be a reason that lower number of patients have lymphadenectomy at RP, as a similar rate for patients with these two kinds of carcinoma undergo a RP. Importantly, more patients with ductal prostate carcinoma have a higher rate of metastasis at diagnosis, significantly. It has not appeared to effect the outcomes of a RP whether patients have a pure ductal prostate carcinoma or admixed ductal and acinar carcinoma (20).
In Epidemiology and End Results (SEER) database from multiple cities and states, 371 out of 442,881 acinar carcinomas (0.08%) were recorded as ductal carcinoma. A previous study of these 371 ductal carcinoma cases showed that they were significantly more aggressive and had a poorer prognosis than the acinar carcinomas in the database. Men with ductal carcinoma had an poorer prognosis and cancer-specific survival outcome when it was compared patients with acinar carcinomas. Ductal carcinomas had similar prognosis to acinar carcinomas with Gleason score 4+4 when acinar carcinoma was stratified by Gleason score to ductal carcinoma However there was an important limit of that study that although the studied had large number of patients, they were not reviewed by urological pathologists. For a case of the problems with some of the SEER data, the Gleason scores were not even mentioned until 2004. As a result, only 30% of the ductal carcinomas in that analysis had a Gleason score, 19% of which were assigned a Gleason score of 6 which has a question the accuracy of the SEER data. Recognizing these limit, the evidence indicated that ductal types could show distant metastasis and lower PSA levels (4, 20).
In the study of Epstein et al, of a group of 18,552 RP specimens obtained at The Johns Hopkins Hospital, almost 93 patients were diagnosed as prostate ductal carcinoma. That research presented that ductal carcinomas mixed with Gleason score 3 had a poorer prognosis than acinar carcinomas with Gleason score 7, moreover the ductal components were >10%. In patients with a small ductal components (10%<), these differences were disappeared (4). This research did not mention any significant differences in the prognosis after RP, possibly because of the relatively small cases examined (n=44). Contrastly, ductal components with the Gleason score 8 to 10 tumors did not show more aggressive than acinar carcinomas with a same Gleason score range. There was also a selection bias in that study advanced ductal carcinomas would not have been considered as RP candidates, therefore they would not been included in the cohorts.
In our current study, we screened an initial cohort of 3,980 radical prostatectomy specimens obtained from 1999 to 2008 at the Asan Medical Center, from which 33 (0.008%) prostate ductal carcinomas were diagnosed. We excluded 3 patients who had lymph node metastasis and 1 patient who had only transurethral resection of prostate. Then we matched with acinar carcinomas from the initial total cohort for biopsy Gleason score, clinical stage, age, and PSA.
There was longer follow-up duration in control group than case group. Because we should investigate old patients for control group among 3,980 prostate acinar carcinoma patients who matched with biopsy Gleason score, clinical stage, age, and PSA.
We found that the only significantly different parameter was the post-surgery Gleason score of ≥8 in ductal carcinomas, which was higher than that in our control acinar carcinoma group (P=0.024). These results are in previous studies ascribing the behavior of ductal carcinoma to Gleason score 4+4 (7).
Additionally we compared biochemical recurrence rate and biochemical recurrence-free survival durations between our two study groups. Kaplan-Meier curve analysis indicated a higher risk of biochemical recurrence in ductal carcinoma. Even though there were no statistical differences between the T, N stage and positive resection margin rate between these two groups, our ductal carcinoma cases showed a much poorer prognosis due to their higher Gleason score.
A noteworthy limitation to our study was that the case and control group patients underwent a radical prostatectomy, which created a selection bias: patients with more advanced ductal carcinoma could not been considered surgical candidates, and we could not have included them in the case group.
Conclusively, even though there were no significantly different clinical outcome in terms of final pathology and positive resection margin rate between our study groups, ductal carcinoma group showed poorer prognosis. Because patients with a greater proportion of ductal carcinoma demonstrated to have more Gleason score ≥8 components in comparison with patients with acinar carcinoma after matching for PSA, Gleason score in biopsy and clinical stage.

 XML Download
XML Download