

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Basaloid squamous carcinoma of the uterine cervix is a rare tumor type characterized by an ulcerated, infiltrating growth pattern; nests or cords of small basaloid cells; prominent peripheral palisading of cells in the tumor cell nests; and the absence of significant stromal reaction (1). These tumors can arise from various anatomic sites, including the hypopharynx, base of the tongue, salivary glands, esophagus, anal canal, prostate, thymus, vulva, and urinary bladder (2-12), but origin of uterine cervix is rare. Basaloid squamous carcinoma of the uterine cervix is neither recognized nor included as a specific histologic subtype in the current World Health Organization (WHO) classification of cervical tumors. Since basaloid squamous carcinomas are thought to behave aggressively (13) but the evidence of supprting this behavior is not powerful, accurate diagnosis and accumulated data of this tumor are important for their clinical management and prognosis.
CASE REPORT
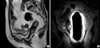
A 70-yr-old woman, gravida 8 para 3, was referred to a tertiary medical center from a local hospital for vaginal bleeding of 3 weeks' duration. She had undergone a punch biopsy at the local hospital, which resulted in a preliminary diagnosis of adenoid cystic carcinoma or carcinoid tumor. Her medical history included diabetes mellitus (DM) for 10 yr which had been controlled by medication; in addition, her mother died of uterine cervical cancer. Physical examination showed uterine cervical erosion. The biopsy specimen taken at the local hospital showed pathologic evidence of a high grade malignant epithelial tumor, with features unusual for a cervical tumor. She therefore underwent a loop electrosurgical excision procedure (LEEP) cone biopsy, which revealed a basaloid squamous cell carcinoma. A colonoscopy, intravenous pyelogram, and cystoscopy showed no evidence of metastatic disease. Magnetic resonance imaging showed a 2 cm sized cancerous mass confined to the cervix, with no evidence of invasion of the vagina or fornix and no evidence of pelvic lymphadenopathy (Fig. 1). The tumor was classified as clinical stage Ib1. A radical hysterectomy was performed, along with bilateral salpingo-oophorectomy, pelvic lymph node dissection, and paraaortic lymph node sampling. The pathologic diagnosis was basaloid squamous cell carcinoma. The depth of invasion was 5/7 mm full thickness of the cervical wall. There was no evidence of tumor in sections taken from 26 lymph nodes. The resection margin of the vaginal cuff was clear. No adjuvant treatment was administered, and the patient was discharged. In the 12 months since discharge, she has shown no evidence of recurrent or metastatic disease. Follow-up is ongoing at Asan Medical Center.
Pathologic findings
A well-defined, fungating firm mass (1.5×1.0×0.6 cm) was present in the posterior wall of the cervix and invaded 5 mm into the cervical wall (full thickness, 7 mm). The parametria and vaginal cuff showed no tumor invasion. The cut surface of the mass was gray and granular. The tumor cells were immunopositive for p63 and immunonegative for S-100 protein. The cells appeared basaloid with small hyperchromatic nuclei, distinct nucleoli and scanty cytoplasm. There was also peripheral palisading, supporting the above diagnosis (Fig. 2).
DISCUSSION
Cervical basaloid carcinoma has recently been classified as a specific histologic subtype, with "pure" basaloid carcinomas being extremely rare (14). Often few incidence of this diagnosis can cause clinical and pathological misinterpretation. In our case, based on a punch biopsy specimen, our patient was initially diagnosed at the local hospital with adenoid cystic carcinoma or carcinoid tumor, which was not an accurate diagnosis. To obtain an accurate diagnosis, an LEEP cone biopsy, which yields a larger tissue sample, was performed and resulted in a diagnosis of basaloid carcinoma of the uterine cervix, indicating that diagnostic difficulties can be avoided by obtaining larger specimens for pathologic diagnosis (15).
The term "basaloid carcinoma of the uterine cervix" refers to any neoplastic lesion of the uterine cervix analogous to a cutaneous basal cell carcinoma (BCC), and may include some of the recognized morphologic variants of BCC. Among the morphologic characteristics of basaloid carcinomas of the uterine cervix are nests or islands of small basaloid cells, hyperchromatic epithelial cells with high nucleus-to-cytoplasm ratios, and a tendency to palisade at the periphery of the tumor islands. A basaloid carcinoma of the cervix may be associated with squamous dysplasia, in situ SCC, or invasive SCC (16, 17).
Immunocytochemistry can occasionally be helpful in identifying the epithelial origin of a basaloid carcinoma of the cervix. Some of these tumors have been shown to be strongly positive for high molecular weight cytokeratin (18, 19), whereas others have shown little or no expression of cytokeratins (17, 20). Most tumors are positive for epithelial membrane antigen (EMA), but show little or no expression of vimentin, smooth muscle actin, desmin or neuroendocrine markers (2, 18, 19).
The major differential diagnosis of basaloid SCC includes the solid variant of adenoid cystic carcinoma (ACC), small cell carcinoma, and large cell neuroendocrine carcinoma (LC NEC) of the cervix. Solid ACC is distinguished from basaloid SCC by the focal presence of basement membrane material enveloped by basaloid neoplastic cells; in addition, the solid variant of ACC may show malignant squamous differentiation. Small cell carcinoma may be composed of variably sized nests of relatively small, hyperchromatic tumor cells, which may mimic adenoid basal carcinoma (ABC) and smaller ABC-like nests. Rare cases may present with large neoplastic islands having peripheral palisading of tumor cells, which may be confused with the solid variant of ACC (21). Small cell neuroendocrine carcinomas may be diagnosed by immunohistochemical or ultrastructural demonstration of neuroendocrine differentiation. Cervical LCNEC, another neoplasm omitted from the current WHO classification of uterine cervical neoplasms, is characterized by large cells with vesicular nuclei and prominent nucleoli, a mitotic index in excess of 10 per 10 high-power fields, geographic areas of tumor necrosis, and positive staining with appropriate immunohistochemical markers of neuroendocrine differentiation (22, 23). Cervical LCNEC composed of large basaloid islands may mimic basaloid SCC, and may also show a considerable degree of morphologic overlap with solid ACC, a lesion that may contain trabecular structures composed of basaloid cells that palisade at the periphery (22). Accurate diagnosis is of prognostic importance because of the biologically aggressive nature of this uncommon type of cervical cancer.
The lack of standard diagnostic criteria for pure basaloid squamous cell carcinoma of the uterine cervix has made it difficult to predict their precise biologic behavior and to design optimal management strategies. Accumulation of data on these rare tumors is therefore necessary to determine whether their behavior differs significantly from that of conventional cervical SCCs of similar clinical stage. Long-term follow-up of this patient and other such patients is therefore important.

 XML Download
XML Download