

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Though occasionally reported, cardiac involvement is a rare phenotypic feature of facio-scapulo-humeral muscular dystrophy (FSH-MD).1) Cardiac involvement in FSH-MD includes cardiomyopathy and arrhythmias.1) Though various arrhythmias have been found in patients with FSH-MD, pre-excitation-syndrome has not been reported.
Case
The patient is a 39-year-old veterinarian who developed slowly progressive muscle weakness and wasting of the shoulder girdle muscles since age 3 years. Initial diagnostic work-up, including muscle biopsy, was non-informative. Since age 29 years he additionally developed diffuse weakness and wasting of the left leg accompanied by muscle stiffness. Since then, he also noted generalized mus-cle tenderness, muscle aching after exercise, and contractures. Cr-eatine-kinase (CK) was repeatedly mildly elevated. Needle-elec-tromyography was myogenic and deoxyribonucleic acid analysis revealed a reduction of the FSH-MD tandem repeat size in the D4Z4 locus on chromosome 4q35 (Fig. 1). Based upon the clinical and genetic findings, FSH-MD was diagnosed at age 30 years. The family history was negative for primary myopathy.
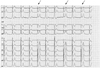
Follow-up investigation in July 2012 revealed a facies myopathica with weakness of the upper lids, inability to voluntarily balloon the cheeks, and weak anteflexion of the head (M5-). There was prominent scapular winging, bilateral diffuse weakness of the upper limbs with right-sided predominance, hypotonia, diffuse wasting, and re-duced deep tendon reflexes. On the lower limbs, there was bilateral weakness of hip flexion (M4) and foot extension (M4-). Patella tendon reflexes were preserved but Achilles tendon reflexes were reduced. There was asymmetric wasting with left-sided predomin-ance, bilateral hypotonia, lumbar hyperlordosis, and a waddling gait. Nevertheless, he was able to play the guitar and drive an automatic car, even over long distances. Cardiologic investigation at follow-up revealed mild myocardial thickening, two intra-ventricular aberrant bands, and, surprisingly, intermittent pre-excitation on routine electrocardiography (Fig. 2). Stress testing to see if there was predominance of prolonged QRS-complexes and thus indication for ablation or predominance of normally-sized QRS-complexes, clearly demonstrated a reduction of prolonged QRS-complexes. Since he was asymptomatic and pre-excitation-syndrome occurred only intermittently, he was not recommended to undergo ablation.
Discussion
The presented case is interesting for the association of pre-excit-ation syndrome and FSH-MD. Rhythm abnormalities so far reported in FSH-MD include impulse generation abnormalities, such as sinus node dysfunction.2)3) supraventricular arrhythmia,3)4) and bradycardia, 3)4)6)7)8) or impulse propagation abnormalities, such as short PR-interval,4) tall P-waves,2)3) abnormal atrio-ventricular conduction with complete atrio-ventricular block,3)4) abnormal Q-waves,8) intra-ventricular conduction delay,3)4)8) incomplete bundle branch block,2) ventricular tachycardia,3) abnormal ST-segment,3) high T-waves,3)4) prolonged QT-interval,6) increased R/S-ratio in V1,7) or hypertrophy.2) In a study of 83 patients with FSH-MD, 12% had cardiac arrhythmias.4) In a study of 24 patients with FSH-MD, 9 had positive ventricular late potentials and increased QT-dispersion compared to controls.9) In the two patients described by Laforêt et al.4) a shortened PR-interval was not associated with a delta-wave.
Discrete concentric thickening of the myocardium was also interpreted as cardiac involvement in the presented case, since the history was negative for arterial hypertension or a thoracic deformity. Single patients with FSH-MD also develop cardiomyopathy.10) Accordingly, echocardiography in FSH-MD may show enlarged right cardiac cavities or restricted right ventricular movement, attributed to thoracic deformities2)8) or hypertrophic cardiomyopathy.4)10) Additionally, myocardial scintigraphy revealed reduced Thallium-201 uptake due to suspected myocardial fibrosis.7)
This case shows that there is indeed cardiac involvement in FSH-MD, manifesting either as hypertrophic cardiomyopathy or arrhy-thmias. Among various different arrhythmias described in FSH-MD, single patients may also develop pre-excitation-syndrome.

 XML Download
XML Download