

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The sirolimus-eluting stents (SES) (Cypher® Cordis, Johnson and Johnson, Florida, USA) and paclitaxel-eluting stents (PES) (Taxus® Boston Scientific Corporation, Massachusetts, USA) are now being used worldwide. They have been approved by the Food and Drug Administration (FDA) for clinical use.1) Both drug-eluting stents (DESs) have been proven to be effective for reducing the rate of restenosis and repeat revascularization in patients who undergo percutaneous coronary intervention (PCI).2)3) However, there are fundamental differences between the SES and PES such as the drug coatings, the polymers and the stent platforms. The stent platform of the Cypher® is the Bx Velocity™ coronary stent (Cordis, Johnson and Johnson, Florida, USA), which uses the closed-cell design. The stent platform for the Taxus® stent and the Express2™ stent uses an open-cell design.1) There is currently limited information on the differences of side branch occlusion (jail) after a PCI procedure between the SES and PES. This is important to determine because events such as a post-procedural myocardial infration (MI) are related to poor clinical outcomes. Therefore, we investigated the rate of side branch occlusion after PCI and the clinical outcomes of patients who received either the SES or the PES for treating de novo lesions of the left anterior descending artery (LAD).
Subjects and Methods
We retrospectively analyzed patients who underwent PCI with SES or PES, after excluding those patients who presented with acute ST segment elevation myocardial infarction (STEMI), non-ST segment elevation myocardial infarction (NSTEMI) and cardiogenic shock. Forty-seven patients who received SES implantation for native coronary lesions were identified (the SES group). These patients were compared with 45 patients who received PES implantation in the same vessel (the PES group). We reviewed the data in the medical records from November 2005 to April 2006 for the patients who underwent one or more DES procedures for the treatment of de novo lesions of the LAD with multiple side branches. We studied the side branches of the LAD that were more than 1 mm in diameter, as noted on the coronary angiograms, to reduce bias.
Coronary angioplasty was performed using the standard percutaneous techniques with the femoral or radial artery approach, and the standard methods were used for stent implantation. All the patients were pretreated with aspirin 100 mg orally before the PCI. Clopidogrel 300-600 mg was also preloaded before the PCI, followed by the daily administration of 75 mg aspirin. The patients were instructed to continue this regimen for 6 months after the procedure. During the PCI, patients received anticoagulation with unfractionated heparin (a bolus of 60 U/kg and then additional heparin to achieve an activated clotting time of 250-300 sec).
All the patients routinely underwent pre- and postintervention 12-lead electrocardiography. The levels of creatine kinase-MB (CK-MB) enzymes and troponin-I were measured from blood samples obtained before the PCI and at post intervention. The measurements were repeated every 8 hr until the peak value was reached and then the values began returning to normal. Patients who already had elevated CK-MB and troponin-I levels above the baseline and before the procedure were excluded from the analysis of postprocedural MI.
Angiographic success was defined as a final residual stenosis <30% with a thrombolysis in myocardial infarction (TIMI) flow of grade 3 or improved. The lesion type (A, B1, B2 or C) was defined according to the modified American College of Cardiology/American Heart Association classification. Stent thrombosis was defined as an occlusion or filling defect at the stent site as documented by angiography, and it was categorized as subacute stent thrombosis (SAT, after the end of the procedure to 30 days post-intervention) and late (late thrombosis, >30 days postintervention).
The angiograms of all study patients were reviewed for the main vessel analysis, the presence of no-reflow phenomenon (transient or final), abrupt closure (transient or final), dissection and distal embolization. Branch occlusion, narrowing and reduction of the TIMI flow at any time after stent placement was recorded for the side branch analysis. The side branch was considered pinched when there was a >50% residual stenosis on the angiogram, including the development of total occlusion or a reduction of TIMI flow more than a grade 1 after the stenting procedures. The Jail Index was defined as the number of occluded side branches or side branches with a reduced TIMI flow after PCI divided by the total number of side branches of the LAD covered by the stents, for the SES or the PES. The occurrence of a postprocedural MI between the two groups was evaluated by the CK-MB and troponin-I levels and the Jail index after the PCI.
Target lesion revascularization (TLR) was defined as a repeat revascularization within the stent or in the 5-mm distal or proximal segments adjacent to the stent. Target vessel revascularization (TVR) was defined as a revascularization of any lesion located in the same previously treated epicardial vessel. Major adverse cardiac events (MACE) were defined as a combination of death, STEMI, NSTEMI, TLR or TVR. The clinical outcomes were evaluated according to the MACEs during the hospitalization and at the 6 month follow up.
Statistical analysis
All continuous variables are presented as mean values ±SDs and these were analyzed using the Student t-test for variables with a normal distribution. Categorical variables are expressed as a percent and they were analyzed 2±2 tables and Fisher's exact test. The statistical software SPSS for Windows (version 12.0, SPSS, Inc, Chicago, IL, USA) was used for all calculations.
Results
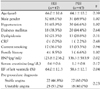
Ninety-two patients were included in the study and analyzed. Forty-seven patients were included in the SES group and forty-five patients were included in the PES group. The mean age±SD of the patients was 66.02±10.6 and 64.15±10.2 in the SES and PES groups, respectively. The proportion of male patients was 68.08% and 68.88%, respectively. The clinical and demographic data was similar in both groups. But the ejection fraction (EF) was low in the PES group and the level of B-type natriuretic peptide (BNP) was high in the PES group (EF: 64.0±12.3 vs. 58.6±12.7, p=0.04, BNP: 125.8±236.2 pg/mL vs. 336.3±583.9 pg/mL, p=0.02) (Table 1).
The coronary angiographic procedures were as follows. The intervention technique was a simple crossover for all stents inserted into the LAD. The number of side branches in the LAD potion where a stent was inserted was 2.00 and 2.13 in the SES and PES groups, respectively (p=0.47). The distribution of the stent sites in the LAD lesion was similar in both groups. The number of inserted stents in the LAD was 1.4 in for the SES group and 1.4 for the PES group. The diameter and length of the inserted stents were 3.0 mm vs. 3.1 mm (p=0.93) and 42.8 mm vs. 41.6 mm (p=0.70), respectively. There were no adverse events related to the PCI such as no-reflow, spasm and perforation in either group (Table 2).
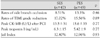
At the end of the procedure, the rate of occurrence of the side branches with a TIMI flow reduction of more than grade 1 was 17.02% and 15.56% in the SES and PES groups, respectively (p=0.89). The rate of side branch occlusion after the procedure was 8.51% and 13.3% in the SES and PES groups, respectively (p=0.46). The rate of side branch occlusion after the procedure was more frequent in the PES group; however, this difference was not statistically significant.
The peak values for the post PCI CK-MB were 13.5 U/L and 15.6 U/L in the SES and PES groups, respectively (p=0.77). The peak values of the post PCI troponin I level were 6.3 ng/mL and 5.42 ng/mL in the SES and PES groups, respectively (p=0.77). As shown above, there were no significant differences in the values of the post PCI peak CK-MB and troponin-I between the two groups.
There was no difference in the Jail index between the two groups; this was 12.4% in the SES group and 12.96% in the PES group. The results of this evaluation showed that there were no significant differences between the outcomes for SES and PES (Table 3).
There were no significant clinical events in the hospital for either group. At the 6 month follow up, there were two patients with MACE in the SES group and four patients with MACE in the PES group (TLR 1:2.1% vs. 3, 6.7%, p=0.47, TVR 1:2.1%, vs. 1, 2.2%, p=0.9, death:1, 2.1% versus 3, 6.7%, p=0.49, respectively, NSTEMI 1, 2.1% vs. 1, 2.2.%, STEMI 0, 0% vs. 2, 4.4%, respectively). One patient in the SES group showed in-stent restenosis and three patients in the PES group showed in-stent restenosis. However, the four patients who died due to adverse events included three patients in the PES group and one in the SES group. The death rate was slightly, but not significantly higher in the PES group (2.1% versus 6.7%, respectively; p=0.49) (Table 4).
Discussion
PCI has been accepted as standard treatment for patients with coronary artery disease. But stenting of coronary lesions sometimes involves the coverage of relatively large side branches that are located near the target lesion. In such cases, there is a risk of side branch compromise (jail) after the PCI. The rate of side branch compromise has been reported to be 3-26%.4)5)
The mechanism of side branch compromise after PCI has not been confirmed. However, several causes have been suggested such as coronary spasms, thrombus formation, atheromatous plaque thromboembolism, dissection and snow-plow effects.6-8) The relationship between the size of the side branches and the rate of side branch compromise has varied. Pan et al.5) reported a higher frequency of side branch compromise in the side branches that were more than 1 mm. However, Iniguez et al.6) and Fischman et al.4) reported different results. In addition, another study found no relationship between the size of side branches and the risk of compromise.10) In several studies, myocardial infarction combined with chest pain after side branch compromise has been reported. However, in most cases there were no significant clinical adverse events.4-6) Therefore, side branch compromise after stent implantation is safe and effective.10-12)
In this study, the angiographic outcomes of compromised side branches (stent jail) after PCI, postprocedural MI and the 6-month clinical outcomes were similar between the patients treated with SES and PES. The in-hospital and 6-month major adverse cardiac event rates were low in both groups despite a conservative treatment strategy for the compromised or occluded small side branches after stenting in the LAD.
There has been concern that the differences in design of the SES and PES may produce different clinical outcomes that cause compromise of the side branches after LAD stenting.1) Experimental data has suggested that closed-cell designs provide a more even distribution of the drug into the vessel wall and fewer cases of plaque prolapses. On the other hand, the open-cell design has better side branch access and stent conformability, and these features may be important in bifurcated lesions.1) At present, there is no data comparing the clinical outcomes of patients treated with SES versus PES stents for compromised side branches after LAD lesion stenting. In our study, the rate of occurrence and the clinical outcomes from compromised and occluded side branches after stent implantation in the LAD were similar in both the SES and PES groups. Although the patients who were treated with the PES had a slightly higher incidence of side branch occlusions and higher values of the peak CK-MB after the procedure, there were no statistically significant differences between the two groups. The Jail index and MACEs at the 6-month follow up were not significantly different on comparison between the two groups. These results suggest that the stent design does not make a significant difference with regard to the side branches of the main coronary artery after PCI procedures. In addition, conservative treatment for compromised or occluded small side branches after stent implantation results in acceptable clinical outcomes.
In a series of 131 bifurcated lesions, the 1-year adverse event rate was 27% and 48% in the patients who underwent balloon angioplasty of the side branch or bifurcation stenting, respectively.13) Similarly, in another series of 92 patients, the in-hospital complication rate was 0% and 13% for the patients who underwent balloon angioplasty to the side branch or bifurcation stenting, respectively.14)15) Another study showed that a conservative approach to side branch management was equally safe compared to bifurcation stenting, and it offered potential cost-saving benefits.1)
The results of our study suggest that for short-term follow up, a conservative approach for small side branch management is safe and acceptable. The influence of different DES implantation devices in the main coronary artery on side branches was similar in our study; we found no difference between the SES and the PES groups. Most of the compromised small side branches had a relatively benign clinical course.
Conclusion
This study was conducted to compare the short-term clinical outcomes and the frequency of an acute side branch occlusion or stent jails between SES and PES procedures in patients with a LAD lesion that included side branches. Our results suggest that the rate of postprocedural compromised side branches and the 6 months clinical outcomes were similar and acceptable between the patients treated with SES and PES for LAD lesion. However, randomized studies with longer follow up and employing a larger patient population are needed to determine the impact of different stent designs on the coronary artery and its side braches.
Limitations
This retrospective study was based on the experience at a single-center that investigated 92 selected patients suffering with chest pain and who had a LAD lesion with side branches diagnosed by coronary angiography; the sample size was relatively small. There was no randomized selection of DESs and the information on the LAD lesions with side branches. We did not evaluate the relationship between the number of stents inserted or the degree of pressure used for the stent implantation and the incidence of side branch compromise.


 XML Download
XML Download