

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Rheumatoid arthritis (RA) is a systemic inflammatory autoimmune disease associated with swelling and pain in multiple joints.1) Despite intensive research, the cause of RA remains obscure. Proposals of the initiating event include an infectious agent or other environmental exposure but genetic, hormonal, and reproductive factors may all contribute to developing RA. RA affects 1% to 2% of adults and, like most autoimmune diseases, develops most often in women, with a female/male ratio of 3:1.2) Previous report reviewed that hormonal involvement is the higher incidence in female RA patients, because disease symptoms lessen during pregnancy and exacerbate in the postpartal period.3) Evidence for endocrine involvement in RA tissue and cells include presence of androgen and estrogen receptors, high concentrations of biologically active steroids, key enzymes of steroid metabolism, and significant changes of estrogen to androgen ratio. These data suggest that individual immune cells, including synovial macrophages, may behave as steroid-sensitive cells.4) Previous studies showed that the immunomodulatory effects of androgens and estrogens may be mediated indirectly.5) One of the best-characterized targets for feedback actions of gonadal steroids is the hypothalamic hormone gonadotrophin-releasing hormone (GnRH).
GnRH is a peptide synthesized and released by the hypothalamus that is responsible for the release of luteinizing hormone (LH) and follicle-stimulating hormone (FSH) from the anterior pituitary. GnRH1 gene located on chromosome 8 p21-11.2 synthesizes precursor GnRH1 protein of 92 amino acids, which is processed to GnRH1 decapeptide in mammals.6) The gonadotroph cells in the anterior pituitary are bathed with pulsatile GnRH which then stimulates its own receptor (GnRHR) to cause secretion of LH and FSH. In females, the acute rise of LH during the LH surge, brought about by the process of GnRH-self priming, triggers ovulation.7) GnRH itself has been shown to be immunostimulatory. Immune cells produce bioactive GnRH and express receptors for GnRH.8-11) Previous studies showed that GnRH exerts stimulatory influences on expression of the interleukin-2 receptor, on B and T lymphocyte proliferation, and on serum IgG levels.12,13) Based on those data, it was hypothesized that differences in responsiveness to GnRH might be due to gender differences in expression of GnRH receptor or due to gender differences in expression of G proteins.13)
We examined five single nucleotide polymorphisms and haplotypes in the GnRH1 regions and their association with susceptibility and severity with RA in female Korean patients.
Materials and Methods
1. Subjects
A total of 153 unrelated Korean female RA patients were participated (Table 1). Each patient was diagnosed by a rheumatologist and diagnosed according to diagnostic criteria, such as erythrocyte sedimentation rate (ESR), C-reactive protein (CRP) and bone erosion. The control subjects (96 female) were recruited after they had been designated as no clinical evidence of RA in a general health check-up program. Written informed consent was obtained from all subjects. This study was approved by the Ethics Committee of Kyung Hee University, Faculty of Medicine.
2. Genotyping
Genomic DNA was extracted from whole blood cells using a Nucleo Spin® Blood kit (Macherey-Nagel, Easton, PA, USA). Five polymorphisms of a GnRH1 gene were selected (Fig. 1). Of the 5 SNPs known to be exist in GnRH1 (http://www.ensembl.org; www.ncbi.nlm.nih.gov/SNP), two SNPs (rs6186, rs6185) were existed in coding region. The corresponding probes were ordered at the company Applied Biosystems, https://products.appliedbiosystems.com (Table 2). Allelic discrimination using fluorogenic probes (5' nuclease assay, Taqman®) was chosen for genotyping on the ABI PRISM 7700 Sequence Detection Systems (Applied Biosystems, Foster City, CA, USA) and consisted of the use of allele-specific fluorogenic probes.14) Twenty nanograms of DNA were amplified by AmpliTaq Gold DNA polymerase which was included in Taqman® Universal Master Mix (Applied Biosystems). The PCR reactions were as follows: one step of 10 min at 95℃ followed by 40 cycles of two-step PCR with denaturation at 92℃ for 15 s and annealing and extension at 60℃ for 1 min. Five percent of all samples were genotyped again for quality control.
3. Statistics
For theses association study, Hardy-Weinberg equilibrium (HWE) for all SNPs was assessed using SNPstats (http://bioinfo.iconcologia.net/index.php).15) A linkage disequilibrium (LD) block of polymorphisms was tested using Haploview (version 4.0).16) The haplotypes and their frequencies were calculated by the EM algorithm.17) Multiple logistic regression models were calculated for the odds ratio (OR), 95% confidence interval (CI) and corresponding p-values, controlling for age as covariables. For all statistical tests, A p-value of p<0.05 was taken as significant.
Results
1. Clinical characteristics of RA in the female Korean
Clinical characteristics of RA patients and control subjects are shown in Table 2. One hundred fifty three female RA patients and 96 female healthy controls were recruited for this study. The mean age in RA patients was 49.3±5.4 years and control subjects 68.9±5.4. The mean disease duration was 4.68±3.53 years. ESR in RA patients was 37.77±26.52 (mm/hr) and CRP was 2.23±6.18 (mg/dL). Seventy three of a total of 153 RA patients exhibited bone erosion (47%).
2. Association between GnRH1 polymorphisms and RA
To assess whether polymorphisms of GnRH1 have any correlation with the risk of rheumatoid arthritis, genotype frequencies of 5 SNPs (rs2659590, rs2321248, rs6186, rs6185 and rs2321049) were examined in 153 rheumatoid arthritis and 96 control subjects, and multiple logistic regression analysis with adjustment for age was done.
Genotype distributions of 5 polymorphisms in this study were in Hardy-Weinberg equilibrium (p>0.05 data not shown). Genotype distributions and allele frequency of 5 SNPs in RA and control subjects are revealed in Table 2 (Table 3). Among 5 SNPs, rs6186 was monomorphic SNP. There was no significant association with RA in genotype distribution and allele frequency between RA female patients and controls (Table 3).
3. Associations between GnRH1 Polymorphisms and parameters of disease activity
As phenotyping stratification, association between polymorphisms and biomarker, ESR and bone erosion was compared as parameters of disease activity.
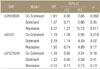
ESR between the ESR 30< and ≥30 was compared (Table 4). Of the five SNPs, 2 SNPs were significantly associated with the risk of RA: rs2659590, OR=4.37, 95% CI=1.21-15.72, p=0.011 in the recessive model; rs6185, OR=1.79, 95% CI=1.09-2.99, p=0.019 in the codominant model and OR=2.29, 95% CI=1.14-4.59, p=0.02 in the dominant model; respectively (Table 5). In the case of rs2321248, there was significant association with ESR level in the G/A genotype; OR=6.67, 95% CI= 1.47-30.16, p=0.0028. Existence of bone erosion was also compared in RA patients. There were no significance in the genotype distribution and allele frequency between bone erosion (Table 6).
4. Associations between GnRH1 Haplotypes and ESR parameter in disease activity
Three among 5 SNPs formed LD block. Haplotypes (frequency>0.01) in the LD block were analyzed using HapAnalyzer software 1.0.18)
Four haplotype were shown. On the haplotype association test, haplotypes, CAG and TGG, showed a significant association between the ESR<30 and ESR 30 RA patients, respectively (Table 7).
Discussion
RA is a common autoimmune disease with a complex etiology in which genetic and environmental factors contribute to disease. The genetic component of RA is largely undefined and, up until very recently, there were only two reproducible associations. The strongest of these associations is of genes within the HLA region, particularly the HLA-DRB1 gene.19) A second, more modest, association identified has been of the protein tyrosine phosphatase non-receptor 22 (PTPN22) gene.20,21) In this study, we demonstrated that whether GnRH1 gene polymorphisms are associated with RA. There was no association between RA susceptibility and GnRH1 in female population.
Altogether the genetics of RA susceptibility has made enormous progress during the past years. In contrast, the field of the genetics of RA severity is relatively unexplored. Radiological joint damage is conceived as the most objective measure to determine the severity of RA. The number of studies investigating the relation between joint destruction and genetic variants is limited. Some SNPs are observed to associate with the disease outcome, but none of these associations are convincingly replicated in independent cohorts. Moreover, although a recent twin study indicated that genetic factors play a role in determining the severity of RA,22) the heritability of the level of joint destruction (the variance of joint destruction that can be ascribed to genetic factors) is still unknown.
Joint damage in RA is highly variable between patients and the cumulative level is associated with the level of (persistent) inflammation. Nonetheless, several studies have provided evidence for incomplete coupling between inflammation and destruction, which suggests that other individual factors also play a role. This suggestion leads to the hypothesis that candidate genes for the severity of RA are, on the one hand, genes that regulate the level of (local) inflammation and, on the other, genes that mediate the process of bone/cartilage destruction or bone regeneration. Gómez-Vaquero et al.23) found significant difference in HAQ scores, ESR, current and accumulated dose of glucocorticoids, and number of disease modifying antirheumatic drugs taken, and lower serum hemoglobin and albumin according to the BsmI VDR gene polymorphisms. For the association analysis of RA-related phenotypes, we assessed whether GnRH1 polymorphisms are related to laboratory markers of disease activity such as ESR and bone erosion. Based on ESR (30 mm/hr) and the existence of bone erosion, we divided the RA patients into two clinical subgroups and analyzed the relationship between clinical data of RA and GnRH1 polymorphisms. Significant genetic associations were found between GnRH1 polymorphisms and clinical data of RA, such as ESR. RA patients were slightly less likely to have elevated ESR/low CRP.24) Infection, renal insufficiency, and low albumin were associated with having elevated ESR/low CRP; low albumin predicted elevated CRP/low ESR and elevated ESR/low CRP discordance. RA patients were less likely to have elevated ESR/depressed CRP. ESR as a measure inflammation in systemic rheumatic disease may be limited in settings of infection, renal insufficiency, and low albumin.
GnRH plays an important role in immune system modulation. GnRH and its receptor are produced locally by immune cells, suggesting an autocrine role for GnRH. Several studies showed that exogenous GnRH stimulates actions in immune response, such as increase the levels of interleukin (IL)-2 receptor, interferon-γ (IFN-γ) and T helper cells. Jacobson et al.13) suggested that GnRH might play a role in the exacerbation of autoimmune disorders. They assessed disease severity in intact and castrated, male and female, systemic lupus erythematosus (SLE)-prone (SWR×NZB) F1 hybrid mice during treatment with a GnRH agonist and antagonist. After 12 weeks of GnRH antagonist administration, total serum levels of IgG and anti-DNA antibodies were reduced, severity of renal disease decreased and survival improved significantly. On the other hand, they also demonstrated sexually dimorphic actions (disease severity was higher in females) of GnRH agonist. Based on their data, these results may partially explain gender differences in immune function.
Summary
In summary, the present study suggests that GnRH1 polymorphisms might not be associated with susceptibility to RA in female population. However, this study suggests that GnR1 gene polymorphisms may play a relevant role in the susceptibility to severity of ESR level in female RA patients. Additional studies, with a larger number of patients and in different populations, may be required to assess whether GnRH1 polymorphisms and these haplotype could be used as susceptibility or resistance markers in RA disease. This study is the first to analyze the association between SNPs of GnRH1 and RA, and may contribute to future studies on GnRH1.







 XML Download
XML Download