

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
As life expectancy increases, elderly colorectal cancer patients are also increasing. Compared to younger patients, the elderly manifest higher co-morbidity with more advanced and emergent disease. However, recent studies have reported similar surgical approaches irrespective of age distribution. We evaluated the outcome and propriety of surgical treatment of colorectal cancer in the elderly.
Methods
The medial records of 464 colorectal patients, who underwent surgery during 2003 to 2007 in Ewha Womans University Mokdong Hospital were reviewed retrospectively. The patients were divided into three groups according to age: I (younger than 70), II (71~80), III (older than 81). Clinical and histological characteristics, surgical outcomes and survival rates were analyzed.
Results
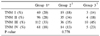
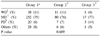
Three hundred and thirty-eight patients belonged to group I, and 104 patients to group II, and group III included 22 patients. Although, male patients were more prevalent in all three groups, female distribution was slightly higher in group III. Clinical characteristics among the three groups did not reveal specific differences except TNM stage distribution. In group I and II, patients with stage II were more common compared to group III, whereas the latter showed most frequently stage III. Histological characteristics and postoperative morbidity rates did not show any difference among the three groups. The survival rate was lowest in group III. However, emergency operation was more frequent in group III, in accordance with increased postoperative complications.
Conclusion
The elderly demonstrated comparable operative morbidity and mortality to the younger patients. Emergency operation was the only significantly influencing factor in the surgical outcome. Therefore, in colorectal cancer patients, surgical treatment in the elderly should be no longer contraindicated.
Figures and Tables
Fig. 1
Complication rate according to age (P<0.05). This figure shows that the Group 3 had the highest complication rate.

Fig. 2
Emergency operation rate according to age (P=0.079). The tendency of the proportion of emergency operation increased in the older group was illustrated in this figure. There is no statistical difference between groups.

Fig. 3
Postoperative complication rate (P<0.05). The postoperative complication rate of emergency operation is higher than the elective one in all studied patients.

Fig. 4
Survival curves according to age. This figure shows that Group 3 had the lowest 5-year survival rate.
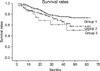
Fig. 5
Survival curves according to curative resection in Group 3 (P<0.05). Survivals in the patients undergoing curative resection were longer than palliative resection.
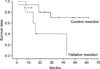
Fig. 6
Survival curves according to chemotherapy in Group 3 (P=0.067). The survival rate of chemotherapy is higher than in the others.



References
1. Programmes and projects; Aging and life course; Facts about ageing [Internet]. World Health Organization. cited 2007 Aug 20. Available from:
http://www.who.int/ageing/en/.
2. Kim JS, Bae SI, Cho MK, Choi ID. Report 2005-15. A Prospect about Long-term Insurance Finance of Old People and Policy. 2005. Seoul: National Health Insurance Corporation.
3. Ministry of Health and Welfare. Annual Report of the Korea Central Cancer Registry 2001. 2003.
4. Ministry for Heath, Welfare and Family Affairs. Annual Report of cancer incidence (2005) and survival (1993~2005) in Korea. 2008.
5. Damhuis RA, Wereldsma JC, Wiggers T. The influence of age on resection rates and postoperative mortality in 6457 patients with colorectal cancer. Int J Colorectal Dis. 1996. 11:45–48.
6. Umpleby HC, Bristol JB, Rainey JB, Williamson RC. Survival of 727 patients with single carcinomas of the large bowel. Dis Colon Rectum. 1984. 27:803–810.
7. Vironen JH, Sainio P, Husa AI, Kellokumpu IH. Complications and survival after surgery for rectal cancer in patients younger than and aged 75 years or older. Dis Colon Rectum. 2004. 47:1225–1231.
8. Patel SA, Zenilman ME. Outcomes in older people undergoing operative intervention for colorectal cancer. J Am Geriatr Soc. 2001. 49:1561–1564.
9. Takeuchi K, Tsuzuki Y, Ando T, Sekihara M, Hara T, Kori T, et al. Should patients over 85 years old be operated on for colorectal cancer? J Clin Gastroenterol. 2004. 38:408–413.
10. Dimick JB, Cowan JA Jr, Upchurch GR Jr, Colletti LM. Hospital volume and surgical outcomes for elderly patients with colorectal cancer in the United States. J Surg Res. 2003. 114:50–56.
11. Bufalari A, Giustozzi G, Burattini MF, Servili S, Bussotti C, Lucaroni E, et al. Rectal cancer surgery in the elderly: a multivariate analysis of outcome risk factors. J Surg Oncol. 2006. 93:173–180.
12. Suh HS, Lee KH, Kim HC, Yu CS, Kim JC. The postoperative impact of co-morbidity in colorectal cancer surgery. J Korean Soc Coloproctol. 2003. 19:299–306.
13. Gonzalez EC, Ferrante JM, Van Durme DJ, Pal N, Roetzheim RG. Comorbid illness and the early detection of cancer. South Med J. 2001. 94:913–920.
14. Anderson JH, Hole D, McArdle CS. Elective versus emergency surgery for patients with colorectal cancer. Br J Surg. 1992. 79:706–709.
15. Biondo S, Pares D, Frago R, Marti-Rague J, Kreisler E, De Oca J, et al. Large bowel obstruction: predictive factors for postoperative mortality. Dis Colon Rectum. 2004. 47:1889–1897.
16. Lee YM, Law WL, Chu KW, Poon RT. Emergency surgery for obstructing colorectal cancers: a comparison between right-sided and left-sided lesions. J Am Coll Surg. 2001. 192:719–725.
17. Kelley WE Jr, Brown PW, Lawrence W Jr, Terz JJ. Penetrating, obstructing, and perforating carcinomas of the colon and rectum. Arch Surg. 1981. 116:381–384.
18. Lee JM, Kim HC, Park IJ, Kim DD, Yu CS, Kim JC. The characteristics of colorectal cancer in patients older than 80 years. J Korean Soc Coloproctol. 2007. 23:490–496.
19. Pavlidis TE, Marakis G, Ballas K, Rafailidis S, Psarras K, Pissas D, et al. Safety of bowel resection for colorectal surgical emergency in the elderly. Colorectal Dis. 2006. 8:657–662.
 XML Download
XML Download