

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Type 2 diabetes mellitus (DM) is associated with an increased loss of skeletal muscle mass and its function during aging [12345]. Though the underlying mechanisms are multifactorial, studies indicate insulin resistance, physical activity status, diet, increased secretion of inflammatory cytokines and oxidative stress may all play a role [67]. Screening to identify muscle weakness and a decline in muscle function (e.g., handgrip strength) among chronic disease-susceptible populations has been pointed as an effective preventative strategy [38].
Some evidence indicates that handgrip strength is associated with DM [35]. However, few statistical adjustments have been taken into account, such as sociodemographic and anthropometric variables. For example, an increase in body weight (adiposity) normally precedes the development of DM and thus research reporting an adjustment of hand grip strength to body weight is desirable. Although a Brazilian study found an association between low handgrip strength (non-normalized by body weight) and DM, this work used odds ratio (OR) analysis only adjusted by age, body mass index (BMI) and physical activity [2], and thus ignored the difference in muscle strength that exist between men and women [135910]. As a result, the association between muscle weakness and DM remains to be fully explored amongst the Brazilian population. We sought to investigate if low handgrip strength is associated with the odds of becoming DM and exhibiting hyperglycemia among Brazilian individuals.
MATERIALS AND METHODS
Study population
A total of 415 (194 male and 221 female) subjects were enrolled in a cross-sectional study. Younger and older adult men and women were recruited in the first semester of 2016 from 5 public parks. The average age of the participants was 45 years (range 19–89 years). Individuals of both sexes who are recreationally active were included. We excluded the subjects who have physical or locomotive problems.
This study was approved by the Ethical Research Committee under protocol No. 1.470.285/2016. All participants signed the informed consent form designed according to the nº 466/12 on “Research involving human beings, from the Health Board of the Ministry of Health.”
Covariates
Demographic, socioeconomic, and lifestyle indicator data were collected through standard questionnaires. Body weight (kg) was obtained using an anthropometric scale (Filizola®; Filizola, São Paulo, Brazil) and height (m) using a stadiometer (SECA®; Seca GmbH, Hamburg, Germany) with BMI (kg/m2) subsequently calculated. All anthropometric measurements were performed 3 times, including arm (cm), mid-arm (cm), and calf (cm) circumferences using an inelastic tape. Handgrip strength (kg) was determined 3 times using a dominant hand trough dynamometer (Takei®; Scientific Instruments Co., Ltd., Tokyo, Japan) and classified for percentile [11]. In addition, the values were normalized to body weight (normalized handgrip strength; NHS) and classified as ‘normal’ or ‘muscle weakness’ (if below of 0.30 for females and 0.46 for males) [35]. All anthropometric measurements were taken by nutritionists previously trained to standardize the collection and minimize error.
Physical exercise routines were self-reported and subjects who reported no structured exercise were classified as sedentary. Thus, individuals who reported more frequent physical activity were classified as ‘recreationally active,’ among the activities more frequent were walking and jogging.
Evaluation of glycemia concentrations
Blood glucose concentrations were obtained using a finger puncture blood sample and measured using reagent strips and a portable automatic monitor (Roche®; Roche Diagnostics, Branchburg, NJ, USA). The glycemia concentrations was measured only once during the park. We considered the measurements to be ‘casual glycemia’ because the evaluation was out of clinic and not controlled for prandial state. DM diagnosis was self-reported by participants. Definition of altered casual glycemia was determined as per the criteria of the American Diabetes Association [12].
Statistical analyses
Data were represented as means and standard deviations and after Kolmogorov-Smirnov test for normality, all statistical analyses were performed. To compare non-diabetic individuals to those with DM, we applied an independent t-test. Fisher's exact test or χ2 test was conducted to verify the difference in smoking status and alcohol intake among men and women.
Logistic regression analysis was used to calculate the OR of individual with low or normal handgrip strength and the association with DM presence or altered casual glycemia. We performed the crude (unadjusted) and adjusted (model 1: exercise frequency; model 2: age; model 3: age and sex; and model 4: age, sex, and exercise frequency) models. All statistical analyses were performed in MedCalc® (MedCalc Software, Seoul, Korea) and considered as significant when a p < 0.05 was found.
RESULTS
From 415 subjects, 9.2% were classified as DM. Diabetic patients showed higher (p < 0.05) age, BMI and casual glycemia, and lower handgrip strength and NHS when compared to non-diabetic patients (Table 1). The logistic regression analyses revealed that low NHS was associated with 2.7 times higher DM presence in crude model (p = 0.006) and 2.7 times after adjusting for exercise frequency (model 1, p = 0.006). However, this association disappeared after adjusting for sex (models 3–4, p > 0.05) (Table 2).
Table 1
General characteristics of non-diabetic and diabetic subjects
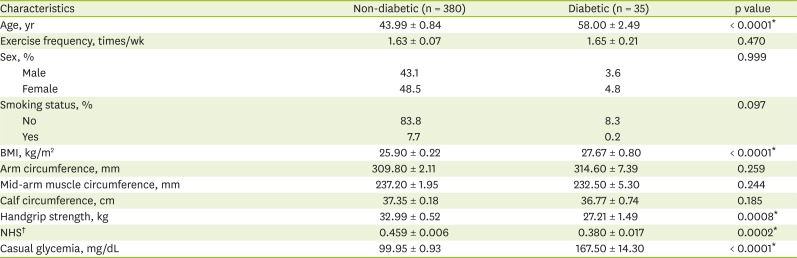
Table 2
Associations of handgrip strength with type 2 DM and hyperglycemia

Data shown are odds ratio (95% confidence interval). Details of each model are follow as: model 1, adjusted by exercise frequency (times/week); model 2, adjusted by age; model 3, adjusted by age and sex; and model 4, adjusted by age, sex, and exercise frequency.
DM, diabetes mellitus; NHS, normalized handgrip strength.
*Handgrip strength is low (muscle weakness) (normal: ≥ p10 or muscle weakness: < p10); †NHS (handgrip strength/body weight, male: < 0.46 or female: < 0.30) is low muscle weakness; ‡Altered casual glycemia was classified when > 200 mg/dL was found; §p < 0.05.
DISCUSSION
In the present study, we showed that low handgrip strength (as a measure of muscle weakness), irrespective of whether normalized to body weight, was not associated with hyperglycemia and/or the likelihood of presenting with DM once data were adjusted for age, sex, exercise frequency, and BMI. This is in line with, and extends on the findings of Leong et al. [9], who did not find any association between low handgrip strength and incidental DM in 2015.
Although there is an evidence which has pointed to a link between hyperglycemia and reduced muscle function [1], our study did not establish such a link, even in a large cohort. A possible explanation is that in our study all findings may be independent of casual glycemia concentrations. In fact, all individuals are park goers and are consequently likely performing at least a modest amount of daily physical activity. In contrast, Amaral et al. [2], also evaluated Brazilian individuals who live in both urban and rural areas of the northern region and found an association of low handgrip strength with DM in 2015. This may be because in the Amaral et al. [2], the individuals possessed a more sedentary lifestyle when compared with our study. Thus, it is suggested that more active lifestyle would lead higher handgrip strength and lower risk of DM. Another difference between the present work and the study of Amaral et al. [2] is the correction for gender. Once the handgrip values are classified according to gender, thus is possible that no correction for gender did not guarantee a direct association among low handgrip strength and DM. Besides, van der Kooi et al. [13] also suggest that ethnic differences may to explain the loss of handgrip strength. Therefore, we speculate that the discrepancies seen in previous studies are better explained by these independent risk factors, rather than hyperglycemia or DM per se.
This study has some limitations. First, the cross-sectional design of the study does not allow a generalization of data to infer causality between muscle weakness and DM, rather, only an association can be established. Second, the casual glycemia was performed in public parks on the weekends, which may introduce substantial variation associated with physical activity status, prandial status, etc.
In summary, low handgrip strength (muscle weakness) normalized or not to body weight, was not associated with self-reported DM diagnosis or altered casual glycemia concentrations after adjusted for age, gender, and exercise frequency.
 XML Download
XML Download