

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Subarachnoid hemorrhage (SAH) is a type of hemorrhagic strokes and is a dangerous disease with high mortality that can cause many serious complications, such as vasospasm, post-hemorrhagic hydrocephalus, and neurogenic pulmonary edema.16)28) Aneurysm clipping, which is a neurosurgical technique, has long been used to treat SAH. Recently, however, a large number of clinicians have begun using aneurysm coiling, which is an endovascular treatment (EVT), instead of aneurysm clipping.17)23) Although most physicians select operation techniques based on the condition of the patient, the location of the aneurysm, or the shape of the aneurysm, controversy still exists regarding the effects of each operation on the occurrence of complications and the outcomes.3)4)5) Delayed hydrocephalus in particular is one of the most common post-hemorrhagic complications after SAH. This condition is known to occur due to obstruction of the cerebrospinal fluid (CSF) pathway or the abnormal absorption of CSF due to hemorrhage.10) However, whether clipping or EVT has a more prophylactic effect on delayed hydrocephalus is still controversial.7)10)
In patients with obstruction of the CSF pathway, lumbar drainage or extra-ventricular drainage (EVD) are performed as additional procedures. Some studies have reported that lumbar drainage is effective in reducing complications such as vasospasm and hydrocephalus by helping to remove the hemorrhage in the basal cistern due to CSF flow.1)20) However, which of the two procedures is more effective in preventing delayed hydrocephalus is still under controversy.19)24)
We investigated whether the operation techniques of clipping or EVT helped reduce the incidence of delayed hydrocephalus. We also determined whether the additional procedures of lumbar drainage or EVD decreased the incidence of delayed hydrocephalus.
MATERIALS AND METHODS
This study was approved by the institutional review board, and the requirement for informed consent was waived.
Patient data
This study was conducted as a retrospective study of patients who visited a single center from January 2012 to December 2015 and who underwent surgery for SAH. Two-hundred and thirteen patients with SAH visited the center. The inclusion criteria were treatment using clipping or EVT operations and a follow-up duration of longer than 3 months after the occurrence of SAH. Five patients who had not undergone surgery, 25 patients who died within 3 months after the occurrence of SAH, and 31 patients who were lost to follow-up less than 3 months after the occurrence of SAH were excluded. Finally, a total of 152 patients were enrolled in this study.
Clinical data
The variables investigated were sex, age, diabetes, hypertension, hyperlipidemia, end-stage renal disease (ESRD), the use of antiplatelet or anticoagulant agents, stroke history, heart disease, Hunter-Hess grade (H-H grade), and operation day (OP day). Information regarding these variables was obtained through a patient chart review. Diabetes, hypertension, and hyperlipidemia were defined as the current use of medication for the respective disease after diagnosis. ESRD was defined as kidney failure (glomerular filtration rate < 15 mL/min/1.73 m2) requiring permanent renal replacement therapy. The use of antiplatelet or anticoagulant agents was defined as the current use of medication, stroke history included both hemorrhagic and ischemic stroke, and heart disease included coronary disease, arrhythmia, and cardiomyopathy. H-H grade was determined according to H-H grade criteria at the initial visit, and OP day was defined as the time between admission and the operation.12)
Procedural data
The surgeon determined the choice of operating technique (clipping or EVT) and whether an additional procedure for CSF drainage was required. In cases requiring CSF drainage, the surgeon chose whether EVD or lumbar drainage should be performed. We recorded the duration that the additional procedure was used for. We also noted whether decompressive craniectomy was required to treat increased intracranial pressure (IICP).
Radiological findings
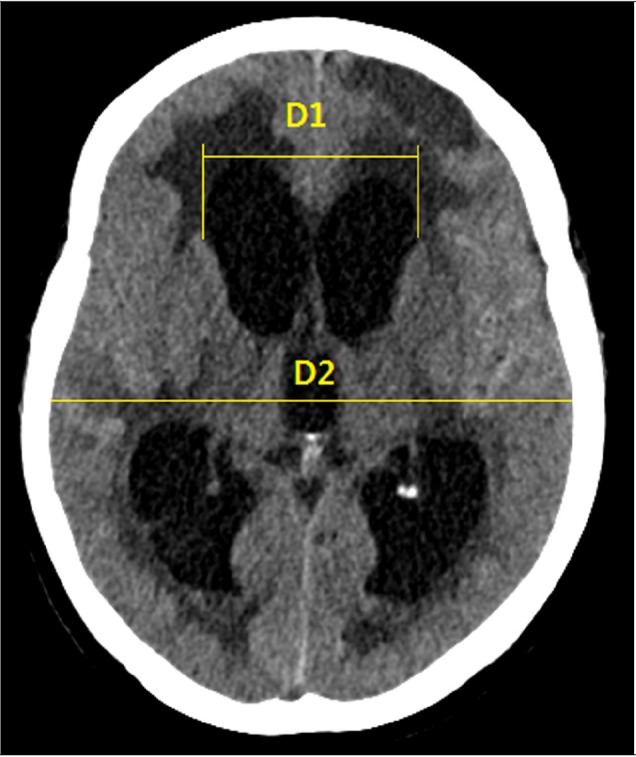
According to the protocol used at our center for patients with SAH, we screened the patient for SAH using brain computed tomography (CT) or CT angiography and performed diagnostic angiography to accurately determine the condition of the aneurysm during the patient's first visit. The location and the maximum diameter of the aneurysm were measured using diagnostic angiography. Fisher grade was determined based on the SAH thickness, as seen on brain CT performed at the time of admission.8) Based on the position of the dominant intraventricular hemorrhage (IVH) as seen on the brain CT performed at the time of admission, the cases were classified as no IVH, or IVH in the lateral, third, fourth, or all ventricles. In addition, when SAH was accompanied by intracerebral hemorrhage (ICH), the ICH was classified as less than 5 mL, 5–20 mL, or more than 20 mL based on ICH volume determined using brain CT performed at the time of admission. Post-operative brain CT was performed immediately after the operation and again 2 days after the operation. Brain CT was immediately performed when neurologic deteriorations were observed. Acute hydrocephalus was defined as an Evan's index of 0.3 or higher as measured on brain CT within 2 weeks after the operation. Delayed hydrocephalus was defined as a condition in which the Evan's index was 0.3 or higher, as measured on brain CT, more than 2 weeks after surgery, requiring shunt placement due to neurological deterioration (Fig. 1).25)27) Vasospasm was defined as a middle cerebral artery (MCA) mean velocity greater than 120 mm/sec or a Lindegaard ratio higher than 3.0 as measured using transcranial Doppler.9) All brain CT and angiography results were reviewed by two independent board-certified radiologists.
Follow-up
Hospital day was defined as the length of hospitalization from admission to discharge. The patient' status was scored at the time of discharge and at the last outpatient clinic visit using the modified Rankin Scale (mRS).29)
Statistics
Statistical analyses were performed using SPSS version 21.0 (IBM Corp., Armonk, NY, USA). Baseline characteristics were assessed and compared between the two groups (“Clipping” vs. “EVT”) using the chi-square test, Fisher's exact test, linear by linear test, or Student's t-test. To assess the association between a risk factor and delayed hydrocephalus, univariate analyses of clinical, procedural, and radiological factors were performed using the chi-square test, Fisher's exact test, linear by linear test, or Student's t-test. Variables with p-values < 0.1 in the univariate analysis were then selected for multivariate analysis. We also selected the operation technique and the additional procedures, which we aimed to investigate, as variables in the analysis. Multivariate analysis was performed using a logistic regression analysis model with a stepwise selection. In all analyses, p-values ≤ 0.05 were defined as statistically significant.
RESULTS
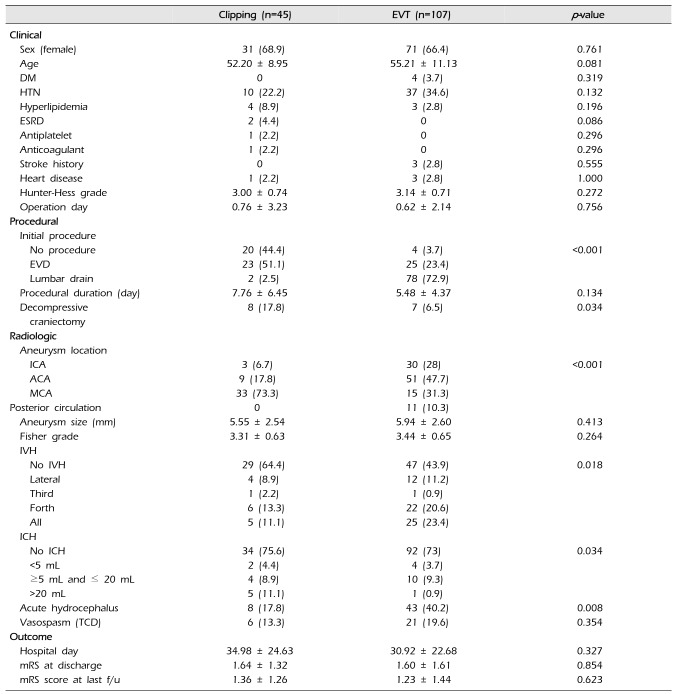
Of the 152 patients, 45 (29.6%) underwent neurosurgical clipping and 107 (70.4%) underwent EVT. There were no significant differences in clinical characteristics between the two groups. However, the use of an additional procedure (p < 0.001) and decompressive craniectomy (p = 0.034) were significantly different between the two groups. EVD was performed more frequently in patients who underwent neurosurgical clipping (n = 23, 51%) than in patients who underwent EVT (n = 25, 23.4%). However, lumbar drainage was performed more frequently in patients who underwent EVT (n = 78, 72.9%) than in patients who underwent neurosurgical clipping (n = 2, 2.5%). Decompressive craniectomy was also performed more frequently in the neurosurgical clipping group (n = 8, 17.8% vs. n = 7, 6.5%). Analysis of the radiological data revealed significant differences between two groups in aneurysm location (p < 0.001), IVH (p = 0.018), ICH (p = 0.034), and acute hydrocephalus (p = 0.008). Patients with MCA aneurysms underwent neurosurgical clipping more frequently (n = 33, 73.3%) than EVT (n = 15, 31.3%). In contrast, patients with posterior circulation aneurysms were only treated with EVT (n = 11, 10.3%). There were more patients with no IVH in the neurological clipping group (n = 29, 64.4%), while there were more patients with IVH in the 4th ventricle (n = 22, 20.6%) and in all ventricles (n = 25, 23.4%) in the EVT group. Analysis of data regarding ICH revealed that most patients in both groups had no ICH (surgical clipping vs. EVT, n = 34 [75.6%] vs. n = 92 [73%]). Among the patients with ICH, the ICHs were larger in the surgical clipping group (< 5 mL [n = 2, 4.4%], 5–20 mL [n = 4, 8.9%], > 20 mL [n = 5, 11.1%]) than in the EVT group (< 5 mL [n = 4, 3.7%], 5–20 mL [n = 10, 9.3%], > 20 mL [n = 1, 0.9%]). There was no difference in outcome between the two groups (Table 1).
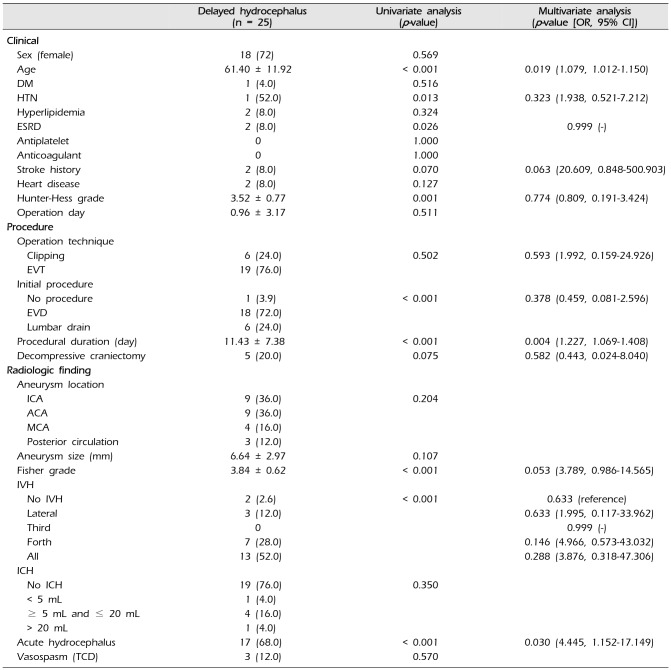
Of the 152 patients, 25 (16.4%) had delayed hydrocephalus. In addition, delayed hydrocephalus occurred in 1 of 31 patients who had not undergone a 3-month follow-up. Among the different factors, age (p < 0.001), hypertension (p = 0.013), ESRD (p = 0.026), H-H grade (p = 0.001), use of an additional procedure (p < 0.001), procedure duration (p < 0.001), Fisher grade (p < 0.001), IVH (p < 0.001), and acute hydrocephalus (p < 0.001) were significantly correlated with delayed hydrocephalus in the univariate analysis. In the multivariate analysis, only age (p = 0.019; odds ratio [OR], 1.079; 95% confidence interval [CI], 1.012–1.150), procedure duration (p = 0.004; OR, 1.227; 95% CI, 1.069–1.408), and acute hydrocephalus (p = 0.030; OR, 4.445; 95% CI, 1.152–17.149) were significantly correlated with delayed hydrocephalus. Stroke history (p = 0.063; OR, 20.609; 95% CI, 0.848–500.903) and Fisher grade (p = 0.053; OR, 3.789; 95% CI, 0.986–14.565) were correlated with delayed hydrocephalus, although the correlation only approached significance were not in fact statistically significant. Operation technique (p = 0.593; OR, 1.992; 95% CI, 0.159–24.926) and the use of an additional procedure (p = 0.378; OR, 0.459; 95% CI, 0.081–2.596) were not significantly correlated with delayed hydrocephalus (Table 2). Patients with delayed hydrocephalus had significantly longer hospital days and poorer mRS scores at discharge and at the last follow-up than those without delayed hydrocephalus (Table 3).
DISCUSSION
Endovascular treatment has recently replaced neurosurgical clipping as the treatment for patients with SAH due to technical advances. In fact, endovascular treatment is now performed more often than surgical clipping.17)23) Currently, the selection of operation technique (neurosurgical clipping or EVT) in patients with SAH is determined based on a consensus regarding operative indications and the benefits and disadvantages of each technique by a large number of physicians.5) Aneurysms in the MCA, which are typical operative indicators, are preferably treated using neurosurgical clipping due to the easy surgical approach.4) However, EVT is preferred for the treatment of posterior circulation aneurysms because they have low surgical accessibility and a high complication rate.3) Because of their locations, posterior circulation aneurysms are frequently accompanied by 3rd and 4th ventricle IVH. Therefore, when patients with posterior circulation aneurysms are treated using EVT, they often develop 3rd and 4th IVH and acute hydrocephalus due to IVH.13)21) Specific characteristics of the shapes aneurysms, such as the presence of a wide neck or a perforating artery in the dome of the cerebral aneurysm, also serve as factors favoring the selection of neurosurgical clipping.5) Furthermore, neurosurgical clipping is preferred when the aneurysm is accompanied by ICH or IICP, as additional operations for hematoma removal or decompressive craniectomy are required in these cases.22)
Our findings regarding differences between patients treated using the two different operation techniques were similar to those of other studies. EVT was frequently performed to treat patients with posterior circulation aneurysms, which were more commonly associated with IVH of the 4th or all ventricles. Acute hydrocephalus was more frequent in these patients. In addition, patients with EVT tended to require additional lumbar drainage. Conversely, neurosurgical clipping was frequently performed in patients with MCA aneurysms, which are easy to access, and in patients with high ICH volume. These patients tended to require additional procedures, such as EVD for the treatment of hydrocephalus or IICP control. However, there were no significant differences in clinical data, initial status, or outcome between the two groups.
Our analyses revealed that old age, procedural duration, and acute hydrocephalus were significant risk factors for delayed hydrocephalus. Fischer grade approached significance, but was not a statistically significant risk factor. We observed no correlations between the choice of operation technique or use of an additional procedure and delayed hydrocephalus.
It is known that post-hemorrhagic hydrocephalus occurs more frequently in old age due to decreased brain elasticity and decreased CSF flow resorption.6)7)15) We confirmed this tendency in our study. This indicated the high reliability of our data. Delayed hydrocephalus tended to occur more frequently in patients with longer procedural durations. In some studies, the procedure duration has been reported to affect the CSF pathway and increase hydrocephalus, and it has been reported that CSF reduces its self-capacity for absorption. Therefore, this study also suggests that procedural duration influences the CSF pathways and self-capacity of CSF absorption, affecting the chronic hydrocephalus.14) Longer procedural durations may have promoted hydrocephalus, although our findings may have been influenced by the inclusion of patients in whom we were unable to discontinue the additional procedure to treat acute hydrocephalus. In a subgroup analysis of 25 patients with delayed hydrocephalus, 10 (40%) were found to have undergone an additional procedure ranging from EVD to lumbar drainage. The procedural duration for this group of 10 patients was 15.50 ± 6.80 days, while the procedural duration for the group of patients with delayed hydrocephalus excluding the above 10 patients was 8.31 ± 6.38 days. There was thus a significant difference between the two groups (p = 0.019). In addition, the procedural duration for the group of patients with delayed hydrocephalus excluding the above 10 patients (8.31 ± 6.38 days) was significantly different from that for the group of patients without delayed hydrocephalus (4.59 ± 2.80 days) (p = 0.041). Furthermore, the procedural duration of patients with acute hydrocephalus (7.45 ± 5.57 days) was significantly longer than that of patients without acute hydrocephalus (4.91 ± 4.08 days) (p = 0.008). These results suggest that not only prolonged procedural duration due to acute hydrocephalus, but also the procedural duration itself, might be affected by delayed hydrocephalus. As a result, restoration of CSF resorption capacity or compensatory mechanisms might be inhibited when longer procedures are used.2)11) Furthermore, acute hydrocephalus might affect delayed hydrocephalus due to not only obstruction of CSF flow, but also increased procedure duration.14)18)
The Fisher grade has been used as an index to measure SAH thickness in the peripheral part of the vessel.8) It is well known that higher Fisher grades are associated with higher risk of vasospasm or hydrocephalus.26) Although the results of this study indicate that Fisher grade was not correlated with delayed hydrocephalus, its correlation with delayed hydrocephalus nearly reached statistical significance.
Limitations
This study has a few limitations. First, our analysis was retrospective in nature. This may have led to selection biases and compounding effects. Second, there were differences in the data according to the operation technique. The location of the cerebral aneurysm, use of an additional procedure, decompressive craniectomy, IVH, ICH, and acute hydrocephalus were significantly different between the two groups. Nevertheless, the differences in most of these factors were consistent with the consensus of the physicians regarding the operation technique. It was not possible to select an operation technique that may have led to a negative outcome for the patients, owing to ethical concerns. Therefore, the above factors were adjusted to correct for biases using stepwise logistic regression analysis. Third, patients with mortality due to the severity of their conditions were not included in the analyses because we only enrolled patients who had undergone follow-up of 3 months or longer in this study. Twenty-five patients in our study died within 3 months of the operation. The missing data from these patients may have led to statistically significant changes in the risk factors for delayed hydrocephalus. Fortunately, delayed hydrocephalus occurred within 2.33 ± 1.66 months among all patients, and was detected in only 1 of 31 patients without follow-ups longer than 3 months. Therefore, we believe that the impact of the patients who had dropped out of the study due to a lack of follow-up is not large. In the future, randomized controlled trials with large samples should be performed to address the above problems and to enable more accurate comparisons. Fourth, Fisher grade and chronic hydrocephalus have been reported to be correlated in a number of studies, but the results are not significant in this study. This is thought to be the result of the small sized study and the bias of the procedure for each treatment.
CONCLUSION
Delayed hydrocephalus was not significantly associated with differences in operation technique (surgical clipping or EVT) in patients with SAH. In addition, there were no significant differences between patients who underwent an additional procedure, no procedure, EVD, or lumbar drainage. However, delayed hydrocephalus was significantly correlated with old age, long procedural duration, and acute hydrocephalus. Therefore, we recommend that additional procedures should be discontinued as soon as possible.

 XML Download
XML Download