

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Early reperfusion of the penumbra area in patients with acute ischemic stroke is critical, for ischemic stroke patients with large vessel occlusion.2)30)31) Recanalization of the occluded artery after intravenous tissue plasminogen activator (IV-tPA) administration is strongly associated with a better neurologic outcome, but large thrombus burden in a large vessel can limit recanalization and increase the risk for hemorrhages.4)13)20)29)32)
IV-tPA administration within a limited time window coupled with non-contrast enhanced brain computed tomography (CT) imaging was the standard treatment protocol.8)9)16)32) Although IV-tPA is effective for recanalizing smaller distal thrombi, dissolving larger more proximal thrombi is not so effective.26) During the last two decades, intraarterial endovascular thrombolytic (IA-Tx) therapy and combined intravenous and intra-arterial tPA therapy have been reported more effective in recanalizaton with acceptable safety standards.4)14)15)21)25) Despite the higher recanalization rate of IA-Tx therapies, no standard therapeutic method for IA-Tx and lack of superiority compared to those of patients who received IV-tPA therapy only.8)15)25) But this idea changed with the publication of the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands, and other reports.4)7)11)12)30)
Although IA-Tx accepted as additional treatment but IV-tPA for indicated patient is still regarded as a first line treatment. We should infused IV-tPA before the IA-Tx if the stroke patient within an indicated time and criteria. Previous reports concern chemical intraarterial thrombolysis, hemorrhagic complication rate increased according to the total amount of thrombolytics.4)10)38) But hemorrhagic complication rate weather IV-tPA or not before the IA-Tx with Solitaire device, has reported as an acceptable complication rate.3)7)11)12)30)
In the Catholic University of Korea, College of Medicne, if a patient arrived within the indicated time, IV-tPA was administered, then underwent acute stroke magnetic resonance imaging (MRI), including diffusion weighted image (DWI), perfusion weighted image (PWI) and MR-angiography, just after IV-tPA administration. And for patients who arrived after the IV-tPA indicated time or who did not demonstrate recanalization after IV-tPA treatment, additional IA-Tx was tried follow the acute stroke MR image. The aim of this study was to analyze the recanalization rate, hemorrhagic complications and clinical outcome of the IA-Tx according to the preceding IV-tPA and perfusion diffusion mismatching (P/D-mismatching).30)
MATERIALS AND METHODS
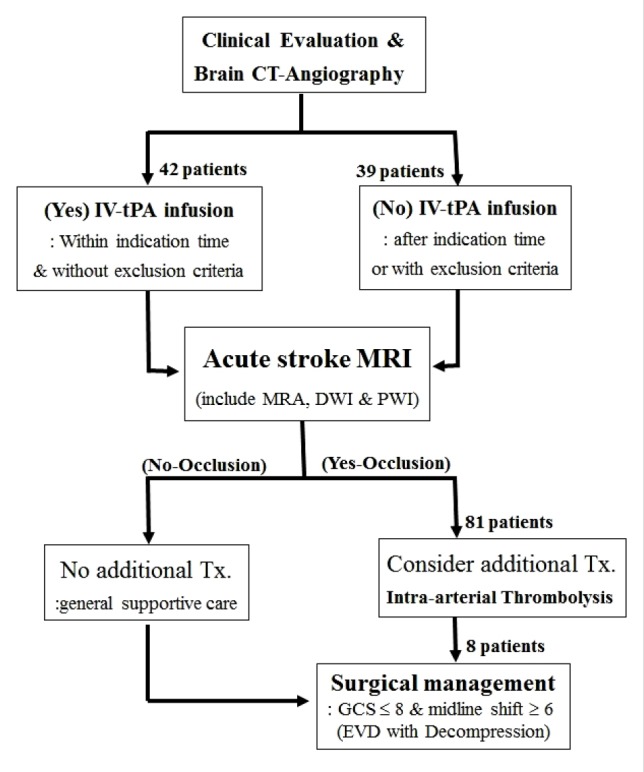
The treatment protocol (Fig. 1) was approved by Institutional Review Board (UC11RISI0187) of the Catholic University of Korea, College of Medicine. All patients or their representatives provided written consent to treatment. Our acute stroke treatment team determined individual treatment approaches based upon each patient's characteristics and findings from CT-angiography and acute stroke MRI.
Patient selection and neurologic examination
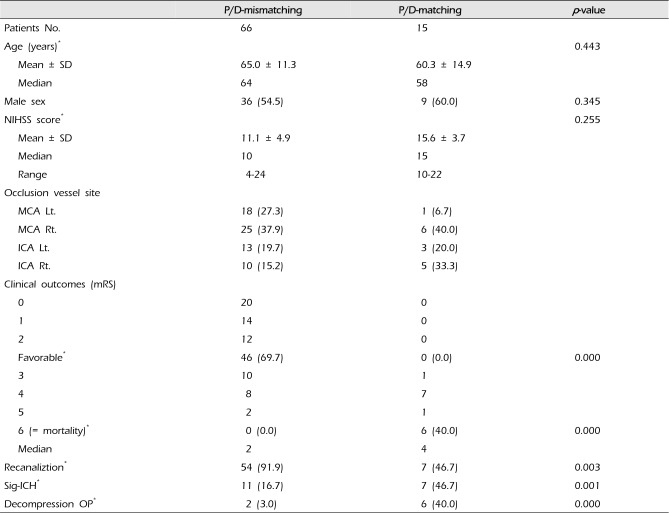
This was a single-center, prospective study that included all patients with acute ischemic stroke who were treated with the Solitaire Flow Restoration (FR) revascularization device (ev3/Covidien Vascular Therapies, Irvine, CA, USA) between August 2012 and August 2016. Eighty-one patients with large vessel, anterior circulation occlusion who treated using Solitaire revascularization devices were analyzed (Table 1). Neurologic status was evaluated using the National Institutes of Health Stroke Scale (NIHSS) at baseline final neurologic status was assessed 90 days after treatment with the modified Rankin Scale (mRS; in which 0 indicates no symptoms and 6 indicates death).
All patients were treated with an antiplatelet or an anticoagulant according to the indications within the first 24 hours after initial thrombolytic treatment. Rehabilitation therapies were started within 72 hours depending upon the patient's condition.
Neuro-radiological evaluations
All patients underwent a CT-angiography (Somatom Definition AS, Siemens Medical Systems, Munich, Germany) as an initial imaging study upon arrival at the emergency room. If a patient arrived within the indicated time for IV-tPA treatment, IV-tPA was administered and an acute stroke MRI (Magnetom Avanto, Siemens Medical Systems) was performed just after the IV-tPA administration. Patients that arrived after the indicated time to receive IV-tPA or with contraindications for IV-tPA, acute stroke MRI was done immediately.
Each patient's radiological results were analyzed by two radiologists, one was not involved in the acute stroke management and one participated in IA-Tx. If the two radiologists reached conflicting conclusions for a patient's images, a third radiologist was consulted. Acute stroke MRI, including T1-weighted axial scans, T2-weighted turbo-gradient axial imaging, spin echo/echo-planar DWI, PWI, and magnetic resonance angiography (MRA) were also obtained. Both DWI and PWI techniques have been described elsewhere.38) A P/D-mismatching profile was defined as a PWI lesion > 120% or more of the DWI lesion.1) Recanalization was measured using TICI score and successful recanalization was defined as TICI grade 2b/3.
Patients who had IA-Tx therapy underwent a follow-up CT study immediately after completing therapy (plain CT) which was repeated within 24 hours (CT-angiography). An increased density on only the original CT image immediately following treatment suggested there was extravasation of the contrast media, but increased density on both follow-up CT scans suggested a hemorrhagic complication. Significant intracerebral hemorrhage (sICH) was defined, according to the European Cooperative Acute Stroke Study I & II criteria, as a hemorrhage seen on the follow-up CT scan associated with an increase in the NIHSS score by 4 points or more.19)
Intra-arterial thrombolysis
IA-Tx was attempted in 222 patients who had large artery occlusions on MRA. Of these, 81 patients were treated with the Solitaire FR revascularization device. Angiographic images (Axium plus, Siemens Medical Systems) were obtained using standard techniques.
Procedures were performed under local anesthesia with mild sedation and maintenance of systolic blood pressure below 160 mmHg. Usually right side groins were prepped and draped in a sterile fashion. The femoral artery was catheterized with an 8-French sheath, and 0.038-inch Terumo guidewire (Somerset, NJ, USA) and a 6-French Cello balloon guide catheter (ev3, Irvine, CA, USA) was introduced to the proximal part of offending occluded artery. The guidewire was removed, the system was flushed, and flow was checked. Multiple runs in multiple views were obtained to look for the site of occlusion. The diseased segment was catheterized highly selectively with a Marksman (ev3) and Synchro 2 (Boston Scientific, Natick, MA, USA). Mechanical thrombectomy was performed using the Solitaire FR device (ev3/Covidien Vascular Therapies). The stent usually deployed and kept in place about 5 minutes then retrieved with aspiration through the balloon guide device. This procedure is repeated until the occlusion site open, some patients failed recanalization or to detach the stent device at the occluded site. Postoperatively, all patients were transferred to the neurointensive care unit after IA-Tx and noncontrast brain CT scan was routinely performed.
Studied variables
Several factors were analyzed to assess their effect on recanalization, complications, and clinical outcomes. These factors include age, sex, NIHSS score on arrival, IV-tPA administration, P/D-mismatching or P/D-matching, and time from onset of symptoms to IA-Tx intervention.
Three end points were considered in this study, clinical outcome evaluated at 90 days after treatment, recanalization grade, and complications after the use of the Solitaire FR device. A poor outcome was defined as a mRS score of 3 to 6 (6 = dead) at 3-month follow-up. A favorable or good outcome was defined as a mRS score of 0 to 2. TICI scores of 2b and 3 were considered successful reperfusion but if the recanalized artery was occluded on the next day CT-angiography, it was regarded as not recanaliation. Complications that were studied included postoperative sICH, reperfusion injury, additional decompression operation and death.
Surgical indication for decompressive craniectomy
In 8 (9.9%) patients, an additional surgical decompression was performed after IA-Tx. The indications for decompressive craniectomy include: the appearance of massive brain swelling on CT scan with clinical deterioration; worsening of the Glasgow coma scale (GCS) score 8 and/or a midline shift of more than 6 mm and/or obliteration of the perimesencephalic cistern on CT scans. We did not perform surgical decompression on patients with primary fatal brainstem failure, as indicated by a GCS score of 3, and/or bilaterally fixed and dilated pupils.18)37)
Statistical analyses
All data are presented as a mean ± standard deviation and/or a median. A Wilcoxon signed-rank test was used to analyze NIHSS scores and mRS. Unpaired t-tests and Fisher's exact tests were used to analyze results between groups.
Statistical analyses for each outcome were analyzed with SPSS software version 20 (IBM Corp., Armonk, NY, USA). For all statistical analyses, significance was defined by a p-value ≤ 0.05.
RESULTS
Patient demographics
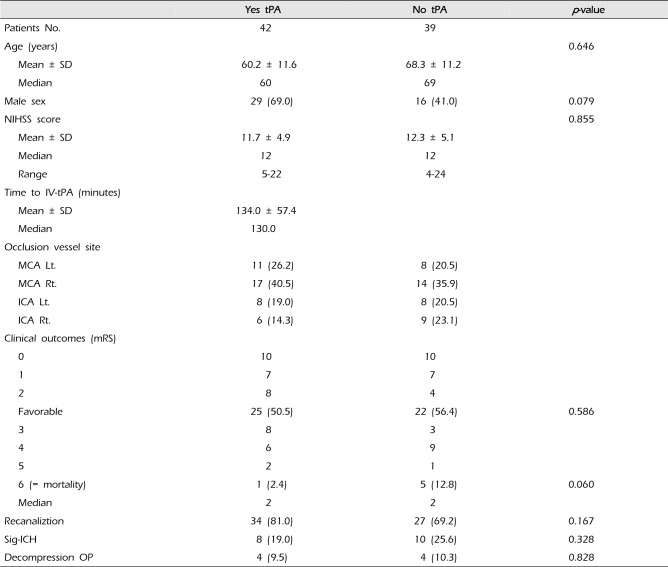
Eighty-one patients with large vessel, anterior circulation occlusion who were treated with Solitaire revascularization devices were analyzed. Patient demographic distributions are summarized in Table 1. The mean patient age was 64.8 ± 12.0 years (median, 63 years) and 45 (55.6%) patients were male. Among these 42 patients were treated IV-tPA and IA-Tx while 39 patients were treated only with IA-Tx, and 66 patients had P/D-mismatching while 15 patients had P/D-matching. The mean initial neurologic status (evaluated with NIHSS) was 12.0 ± 5.0 (median, 12). The mean time to IV-tPA administration (42 patients who treated IV-tPA) after stroke symptom onset was 134 ± 57.4 minutes (median, 130 minutes) and time to femoral artery puncture was 6.0 ± 2.7 hours (median, 6 hours).
Clinical outcomes according to whether preceding IV-tPA
In patients who were treated IA-Tx after receiving IV-tPA, the recanalization rate was 34 (81.0%) and the sICH rate was 8 (19.0%), while these rates were 27 (69.2%) and 10 (25.6%) in patients who were treated with IA-Tx without IV-tPA (p = 0.167 and p = 0.328, respectively; Table 2). Neurologic outcomes were not statistically significant between the IV-tPA treated and non-treated groups (p > 0.05; Table 2).
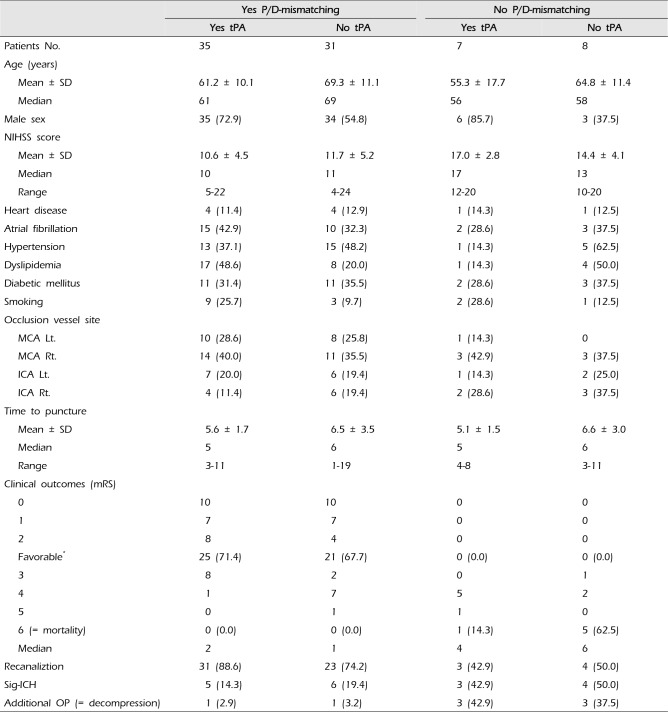
Clinical outcomes according to weather P/D-mismatching
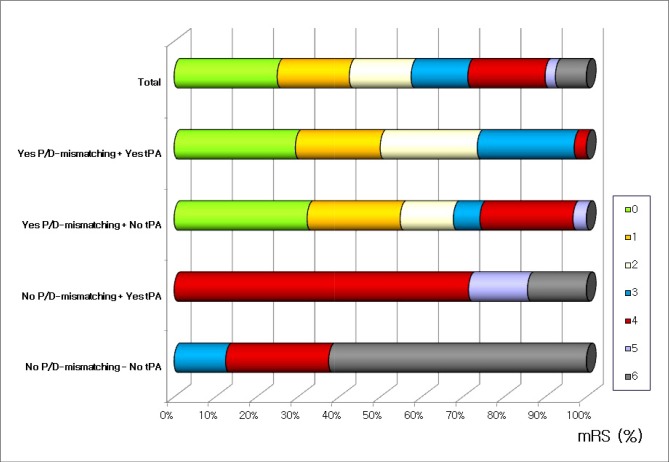
The mean initial neurologic status (evaluated with NIHSS) was 11.1 ± 4.9 (median, 10) in P/D-mismatched patients while it was 15.6 ± 3.7 (median, 15) in P/D-matched patients (p = 0.255). The recanalization rate was 54 (91.9%) and the sICH rate was 11 (16.7%) in P/D-mismatched patients, while it was 7 (46.7%) and 7 (46.7%) in P/D-matched patients (p = 0.008 and p = 0.019, respectively, Table 3). Neurologic outcomes for P/D-mismatched patients, 46 (69.7%) patients was favorable, and no patients died, but 0 (0%) had a favorable outcome and 6 (40%) died in P/D-matched patients (p = 0.000 and p = 0.001, respectively; Fig. 2).
Hemorrhagic complications
In patients who were treated with IA-Tx prior to IV-tPA, the sICH rate was 8 (19.0%), while it was 10 (25.6%) in patients who did not receive IV-tPA (p > 0.05; Table 3). The sICH rate was 11 (16.7%) in P/D-mismatched patients, while it was 7 (46.7%) in the P/D-matched patients (p < 0.05; Table 2). In IA-Tx with retrieval stent, IV-tPA treatment had no influence on the sICH incidence (χ2, p = 0.328).
Additional decompression surgery
In 8 (9.9%) patients, all of the surgery indicated patient, an additional surgical decompression was performed after IA-Tx. Among these patients, 2 (3.0%) patients showed P/D-mismatched and 6 (40.0%) showed P/D-matching (p = 0.000). Of these patients 4 (9.5%) were IV-tPA treated and 4 (10.3%) patients did not receive IV-tPA (p = 0.601).
DISCUSSION
The main goal of cerebral ischemic stroke treatment is reopening of the occluded vessels before the critical cell damage happens. Recanalization of the occluded artery may allow reperfusion and improve the clinical outcome by saving vulnerable tissues namely the ischemic penumbra.2)8)25)
Until the end of 2014, the only specific therapy for acute ischemic stroke was IV-tPA up to 4.5 hours after symptom onset. However, patients with occlusions of large, proximal, intracranial arteries are not typically responsive to IV-tPA, early reperfusion occurs in only 13–50% of patients with occlusions in the ICA terminus and the proximal segment of the middle cerebral artery.26)30) Furthermore for the limitation of time and the numerous exclusion criteria for IV-tPA, only about 10% of patients meet the current eligibility criteria for receiving IV-tPA.8)9)16)32) Because of these limitations of IV-tPA therapy, IA-Tx therapy or combined IV-tPA plus IA-Tx have been tried and reported to have a recanalizaton rate over 80–90% with acceptable safety.4)12)14)15)21)25) Despite the higher recanalization rate of these therapies, the neurologic outcomes of the stroke patients have not been shown to be superior compared to those of patients who received IV-tPA therapy only.8)15)25) And some reports concern chemical intraarterial thrombolysis, said that hemorrhagic complication rate is high and this hemorrhagic complication increased according to the total amount of thrombolytics.4)10)38)
Non-contrast CT is the mainstay of imaging in suspected acute stroke patients. However, advanced dynamic imaging techniques such as CT-angiography and acute stroke MRI have become important tools for identifying vulnerable ischemic tissue.1)5)6)13)15)16)36) It is becoming more and more important to evaluate the ischemic tissue viability because therapeutic interventions may eventually be individualized to a patient's unique physiologic state.1)22)24) MRI imaging is reasonable to be able to identify patients who may still benefit with reperfusion at later time points. Some studies commented on merit of MRI based individualized patient selection.7)23) P/D-mismatching on acute stroke MRI may signal tissue that is at risk for cerebral infarction namely the ischemic penumbra, if blood flow is not restored to the area.1)6)10)14)22)24)25)26) Although P/D-mismatching is an imaging selection tool for use in patients with acute ischemic stroke, there are some practical drawbacks. DWI imaging provides the most accurate assessment of the ischemic core, but the time taken to screen the patient for metallic implants and access to the scanner also needs to be considered. In this study, the authors found that, although beyond time to IV-tPA, some P/D-mismatched patients showed recanalization, low hemorrhagic complication rate and favorable outcome.
Some reports concerned hemorrhagic complications, it strongly correlated with a patient's age, clinical stroke severity, having high blood pressure, having hyper-glycemia, showing early CT changes, and signs of leukoaraiosis on MRI.20)27)28)34)36) Previous reports that explored the hemorrhagic complication rate after IA-Tx treatment, with or without IV-tPA infusion, did not focused on the hemorrhagic complication.5)8)25)38) Authors previous reports, IA-Tx with chemical or combined chemical and mechanical IA-Tx, patients treated IA-Tx after IV-tPA infusion, both recanalization rate and hemorrhagic complication rate increased.35)38) But in this study, IA-Tx with stent retriever, hemorrhage complication was not increased by preceding IV-tPA infusion (p = 0.161), rather it was correlated with P/D-mismatching (p = 0.001).
The mortality rate was somewhat low in this study. Decompressive surgery might be helpful for decreasing the mortality caused by major stroke, even though it may not improve neurologic outcomes for survivors.4)8)12)13)17)33)35) Decompression surgery in proper time should be performed to improve the neurologic outcome for acute stroke patient caused by the larger vessel occlusion.
CONCLUSION
As previous reports, P/D-mismatching was correlated well with the recanalization rate, hemorrhagic complication rate and clinical outcomes. In our study, also confirm the clinical significance the P/D-mismatching. And authors would like to insist that IV-tPA infusion before the IA-Tx, did not increase hemorrhagic complication rate.
 XML Download
XML Download