

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Kissing aneurysms arising from a proximal basilar artery (BA) fenestration are extraordinary and posing therapeutic challenges.5)8) In terms of safety, the endovascular approach may be more reasonable than the surgical approach for treatment of this pathology locating in critical brainstem region. Development of self-expanding stents and advancement of stent-assisted techniques have broadened the scope of endovascular treatment for the more complex aneurysms once thought uncoilable. The authors describes the successful endovascular treatment using double-barrel stent-assisted coiling with dual closed-cell stents for kissing aneurysms at the proximal junction of the basilar fenestration with a wide base incorporating both limbs of the fenestration and distal vertebral arteries (VAs).
CASE REPORT
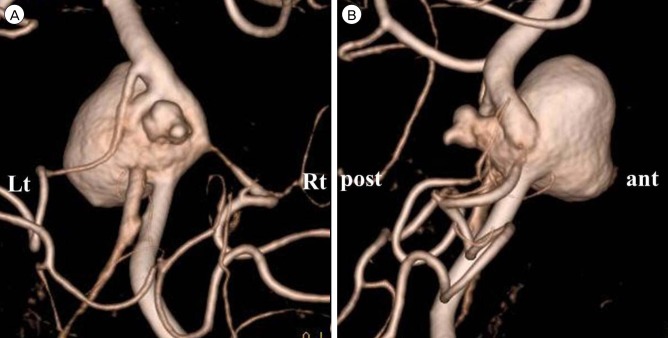
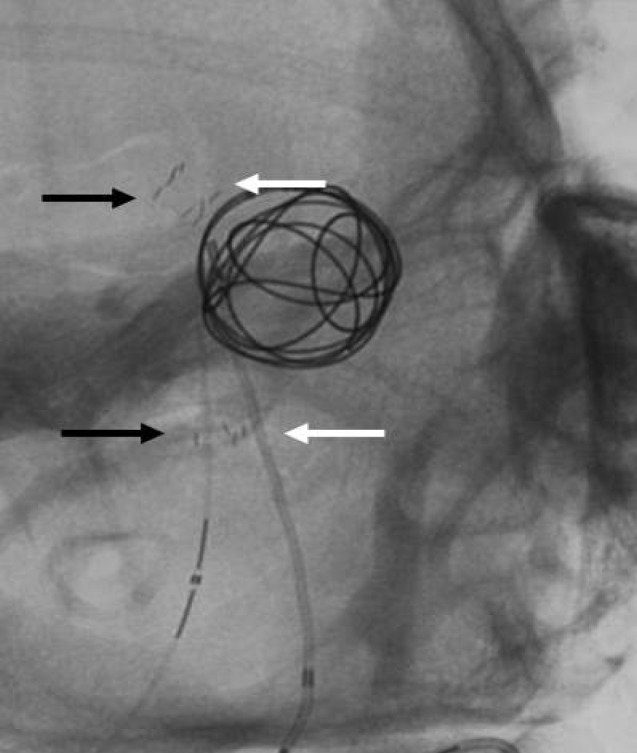
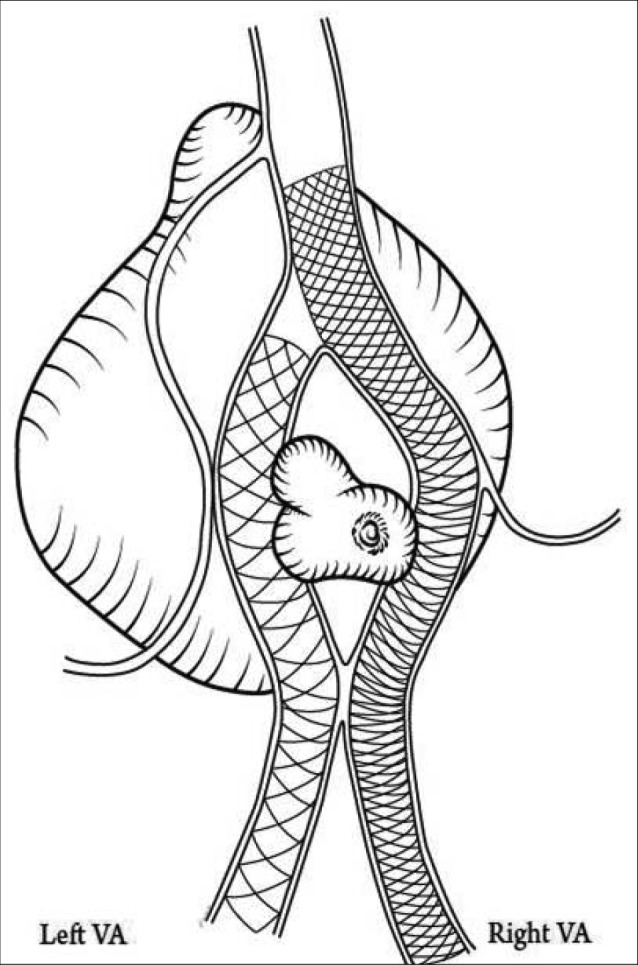
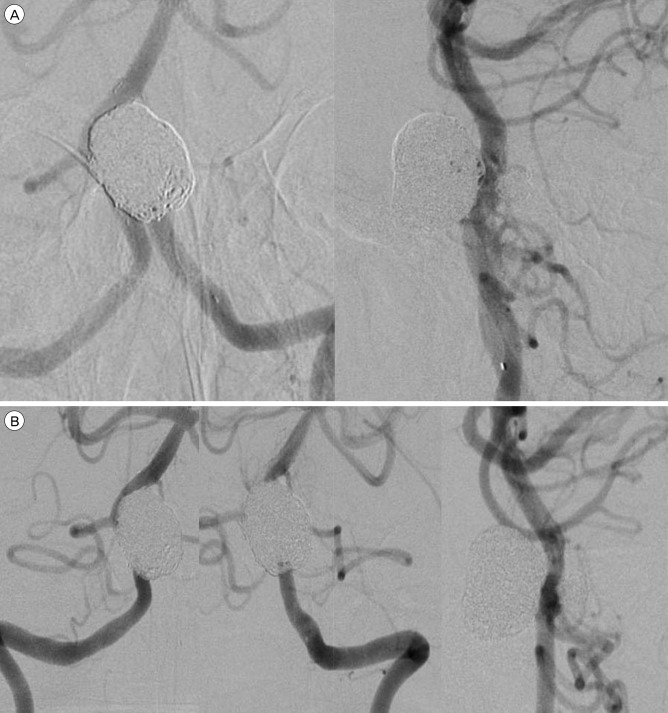
A 51-year-old woman presented with an unruptured aneurysm located in the proximal basilar region found on the computed tomography angiogram. Three dimensional reconstruction of cerebral angiography showed two discrete aneurysms adjoining each other at the proximal junction of the proximal basilar fenestration with a wide neck incorporating both fenestrated limbs and both distal VAs. A single trunk of the right anterior inferior cerebellar artery (AICA) - posterior inferior cerebellar artery (PICA) originated from the right fenestrated limb. The larger aneurysm, measuring 16.2 × 12.3 mm in size, directed ventrally, while the smaller one, measuring 5.2 × 4 mm, dorsally, with an irregular tit (Fig. 1). The patient received dual antiplatelet therapy with oral aspirin (300 mg/day) and clopidogrel (75 mg/day) 1 week before the procedure. The procedures were performed using the bilateral transfemoral approach under local anesthetic and systemic heparinization. A 5Fr guiding catheter (Envoy; Cordis, Miami Lakes, FL, USA) was advanced and placed in both distal VAs. A Prowler Select Plus microcatheter (Codman Neurovascular) was advanced to the distal BA via the right side fenestrated limb through the guiding catheter in the right distal VA. Same procedure was performed opposite side with a Rebar (ev3, Irvine, CA, USA) microcatheter. A 4.5 mm × 22 mm Enterprise closed-cell stent (Codman Neurovascular) was initially deployed from the right side fenestrated limb to the right parent VA. Then, a microcatheter (Headway; MicroVention®TERUMO) for delivery of coils was navigated via an Enterprise stent interstice into the large aneurysm through the right guiding catheter, followed by deployment of a 4 mm × 20 mm Solitaire AB stent (Covidien, Dublin, Ireland) from the left side fenestrated limb to the left distal VA in a double-barrel configuration (Fig. 2, 3). After successful deployment of the stents, the larger ventral aneurysm was coiled completely. After the occlusion of the larger aneurysm, the other smaller aneurysm was selected by re-navigation of the microcatheter without any difficulties and coiled completely. The final angiogram depicted complete aneurysm obliteration and preservation of both fenestrated limbs as well as both parent VAs (Fig. 4A).
There was no occurrence of periprocedural complication. Administration of the dual anti-platelet agents continued for six months after the procedure, and the patient remained on aspirin indefinitely. Angiography performed at the 12-month follow-up demonstrated persistent complete obliteration of the aneurysms with patency of both limbs and no evidence of in-stent stenosis (Fig. 4B). The patient has been well for a clinical follow-up period of 5 years.
DISCUSSION
Kissing aneurysms of proximal basilar artery fenestration have important characteristic findings for treatment.3)5)8) First, the aneurysm neck is usually broad and is incorporated with both fenestration limbs and both distal parent VAs. Second, two kissing aneurysms are asymmetric in size and are not clearly delineated from one another. In our presented case, these all characteristics were presented. Besides, the AICA-PICA trunk originates from the right limb of the fenestration, and angiographic occult brainstem perforators can originate from both limbs and distal vertebral arteries, the flow patency of these arteries is prerequisite to preventing infarction of brainstem and cerebellum. Some viable stent techniques, such as X-configuration stent, Waffle-cone, and single crossover stent-assisted techniques, for coiling of wide-necked aneurysms associated with fenestration have been suggested. Use of a single crossover stent-assisted technique was limited due to the high possibility of an inadequate scaffold for protection of the wide neck incorporating both bifurcated arteries. The waffle-cone technique is one possible option.2) However, it lacks durability due to serving to direct jet flow into the coiled aneurysm.1)10) X-configuration stent technique guaranteed excellent neck remodeling of a wide neck aneurysm, complete aneurysm occlusion, low recurrence due to the flow diverter effect, and maintained sufficient flow patency of parent arteries in the reported cases.7)9) However, possible failure of microcatheter re-navigation into the other aneurysm after coiling of the first aneurysm by tangled struts of crossed stents is expected. In addition, demerits of this technique are potential risk of undesirable stent migration or malposition due to stent-to-stent interference and thromboembolic risk related to overlapping stents as well.6)
Compared with X-configuration stent technique, parallel stent deployments in the double-barrel stent-assisted coiling enable easy advancement of a microcatheter through the vessel and good stent-vessel wall apposition without substantial mutual interaction between two stents, facilitating successful coiling and lowering the risk of thromboembolic events respectively. The complete retrievable Solitaire AB was selected for the second stent in the presented case as a safety net to enable easier navigation of the microcatheter into the last aneurysm in sequential coiling.
Most recently, Kan and colleagues4) introduced double-barrel stent-technique using mixed stents (closed/open-cell stents) for coiling of a single aneurysm arising from basilar fenestration, focusing on its simplicity and safety. In our case with two adjoined aneurysms to be coiled, use of an open-cell stent is not optimal due to its irretrievability. When catheterizing the other aneurysm after coiling of the first aneurysm, stent struts can hinder navigation of the microcatheter. In such cases, struggling to catheterize into the aneurysm may increase the risk of perforation, especially in the small aneurysm. Therefore, use of retrievable stents is quite advantageous in such case in terms of providing a safety net.
 XML Download
XML Download