

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
The A1 segment of the anterior cerebral artery (ACA) usually arises from the internal carotid artery (ICA) bifurcation and extends anteromedially above the optic nerve or chiasm to join the anterior communicating artery (ACoA). Variations of the ACA-ACoA complex are commonly identified in aneurysm surgery. An infraoptic course of the ACA is exceedingly rare. Robinson first described this anomaly from an anatomic dissection in 1959.12) A unilateral anomalous infraoptic ACA is more common than anomalies of bilateral infraoptic ACAs.4) We report on the case of an unruptured AcoA aneurysm in a patient with bilateral infraoptic ACAs. Implications for aneurysm formation and surgical treatment are discussed.
CASE REPORT
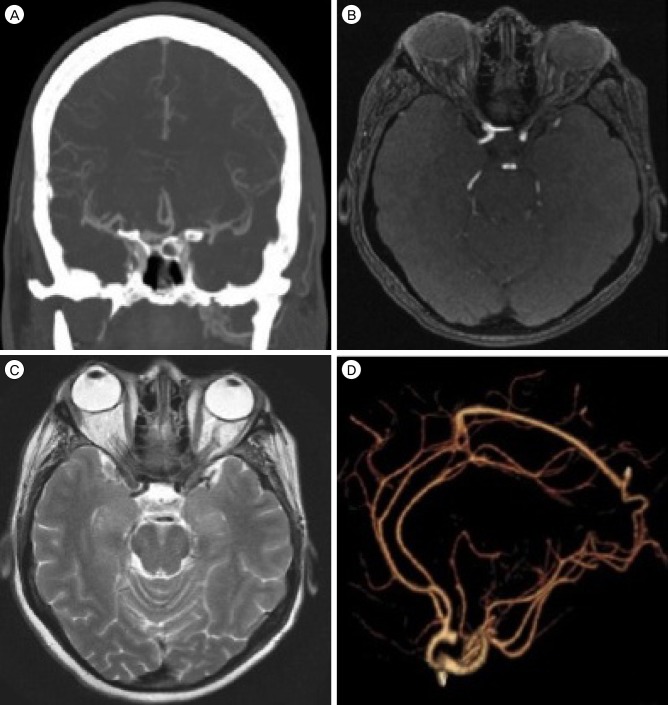
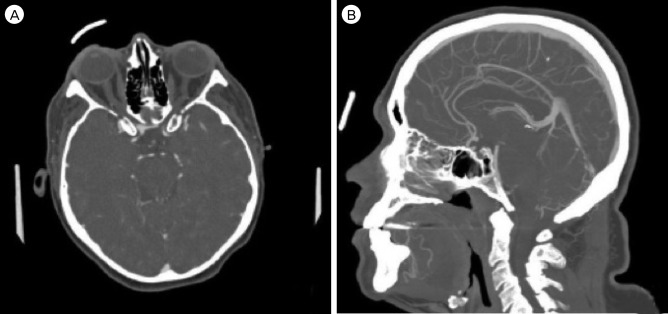
Our patient developed symptoms of episodic left arm twitching. His family history included significant intracranial aneurysms. Imaging demonstrated a 5-mm ACoA aneurysm which projected posteriorly with early bifurcations of the ICA bilaterally (Fig. 1, Fig. 2). The A1 segments were identified as they traversed the pituitary fossa in an unusually low and laterally directed course, indicating their infraoptic nature.
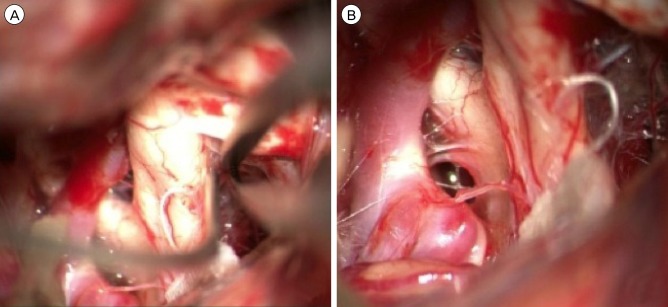
Discussion with the patient resulted in the decision to proceed with clip obliteration of the aneurysm due to significant family history and extreme anxiety regarding the diagnosis. A standard right pterional craniotomy was performed and as the optic nerve was exposed for CSF drainage, the infraoptic course of the ipsilateral A1 became visible. The contralateral A1 was then exposed and showed the same course across the skull base (Fig. 3). Once proximal control was defined, the ACoA was exposed along with the bilateral A2 segments. As predicted by the preoperative CTA, the aneurysm projected posteriorly. Both A2 segments projected anteriorly and swept around the base of the lesion. Each of the recurrent arteries of Huebner arose from its typical location in the proximal A2 segment. Proximal control with bilateral A1 temporary clipping was performed and final aneurysm dissection with neck preparation was achieved. The aneurysm was clipped uneventfully, the temporary A1 clips were removed, and ICG video angiography was used to identify aneurysm obliteration and preservation of the parent vessels. The patient was discharged home on post-operative day 2. Overall post-operative course was uneventful.
DISCUSSION
An infraoptic ACA is associated with a low bifurcation of the ICA and suggests abnormal development of the circle of Willis.13) This has been associated with other coexisting vascular anomalies including normal ACoA complex with an additional infraoptic vessel that forms an anastomosis between the ICA and ACA; absent ipsilateral or contralateral A1; early bifurcation of the ICA at the level of the ophthalmic artery; and termination of an accessory infraoptic ACA in normal frontal brain parenchyma in the presence of a normal ACoA complex.
Bilateral infraoptic ACAs are less common than unilateral anomalies.8) One report describes an associated gyral abnormality.11) The anomalous ACA usually arises from the intra-dural ICA near the level of the ophthalmic artery, as it did in the presented case, or rarely from the extra-dural ICA.9)
The most important clinical association of such an anomaly is the high incidence of intracranial aneurysms of the ACA-ACoA complex.5)8)14) Recognition of this anomaly is important in planning surgery for ACA-ACoA complex aneurysms in order to identify proximal arterial control of the aneurysm. Failure to account for this anomaly might result in unnecessary dissection along and possible damage to the optic apparatus or inferior frontal lobe during aneurysm repair. In the case of this anomaly, surgical treatment of the aneurysm at the ACoA may be difficult because the proximal ACA may be obscured by the optic nerve. In addition, the altered course of the A1 may change the orientation of the ACoA complex (and thus its important perforators which normally project posteriorly) or the Artery of Heubner as it arises from the proximal A2 or distal A1. Careful radiographic evaluation and understanding of variations of the ACA are essential for surgery. In this case, pre-operative knowledge of these anatomic variants enabled early identification of the ICA bifurcation under the optic nerve and unnecessary dissection along the inferior frontal lobe or optic apparatus was avoided. In this case, given the early medial infraoptic course of the A1 arteries, establishment of proximal control was comparatively easy.
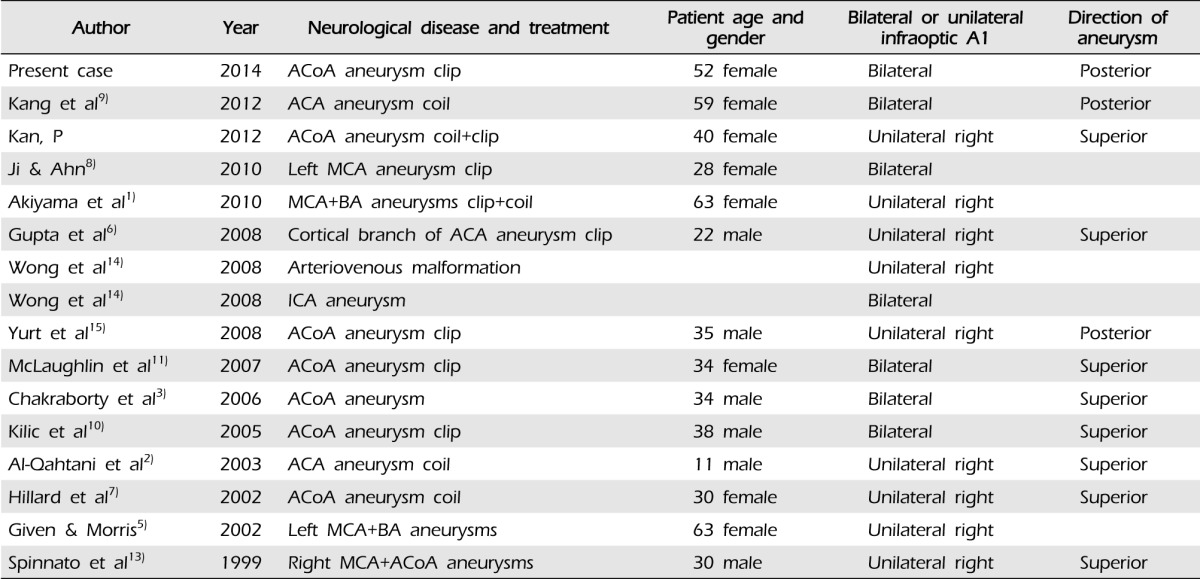
Pre-operative evaluation of the ACoA complex anatomy is critical in the clipping of an ACoA aneurysm (as it is for any aneurysm location). Exposure of aneurysms located more than 1 cm above the skull base will be more difficult due to increased need for frontal lobe retraction as well as possibly interhemispheric dissection and gyrus rectus resection just to visualize the aneurysm. In addition, clipping of posteriorly projecting ACoA aneurysms is typically more difficult as the aneurysm projects in the same direction as the important perforator arteries. A posterior projecting aneurysm is often found in cases of an infraoptic A1 given the course of the ACA from inferior to superior as it turns under the optic nerve towards the ACoA complex (Table 1). However, in the reported case, the unusually anterior location of the ACoA complex actually made aneurysm exposure easier. In addition, the perforating vessels from the ACoA were pushed above the lesion, making safe surgical clipping without compromise of the associated perforating arteries more likely.
CONCLUSION
Safety in surgical clipping of intracranial aneurysms is achieved through many steps. Thorough pre-operative evaluation of the aneurysm as well as its parent vasculature is critical to achieving good surgical results. An infraoptic course of A1 from an early ICA bifurcation is rare; bilateral infraoptic A1 courses are even rarer. A pre-disposition to ACoA aneurysms appears possible with an infraoptic A1 course given the previous reports of association as well as this case. Identification of this anomaly pre-operatively can enhance surgical safety in aneurysm clipping and unnecessary and potentially dangerous dissection can be avoided.
 XML Download
XML Download