

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Vertebrobasilar fusiform aneurysm (VFA), also known as vertebrobasilar dolichoectasia, is a vasculopathy characterized by pathologically elongated and dilated vertebral and basilar arteries with estimated incidence of 0.06 - 5.8%.10) It can be diagnosed radiographically using Smoker's Criteria.8) Clinical manifestations of VFA may include ischemic stroke, cranial nerve palsies, brainstem compression, hydrocephalus and intracranial hemorrhage.6)10) Subarachnoid hemorrhage (SAH) is an uncommon presentation of VFA with a crude incidence rate of 2.2 per 1000-person years.6) Traditional treatment options for ruptured VFAs have been limited and often carry significant mortality and morbidity.
The Pipeline embolization device (PED) (Covidien, CA) is a braided, self-expandable, platinum and nickel-cobalt chromium alloy wire mesh initially approved by Food & Drug Administration (FDA) for treatment of aneurysms in the internal carotid artery from the petrous to the superior hypophyseal segments. PED is considered a flow diverter. Since its FDA approval, PED has gained much popularity in an attempt to reconstruct vessels with abnormal morphology. Several centers have reported using PED for treating complex posterior circulation aneurysms with mixed results.1)5)7)9) In this report, we describe the use of PEDs to successfully treat a ruptured VFA.
CASE REPORT
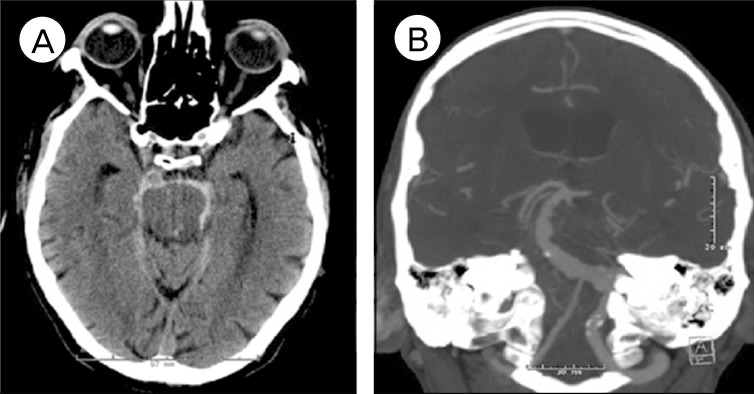
A 73-year-old man presented with Hunt and Hess II SAH. There was no radiographic or clinical evidence of hydrocephalus on admission. He was on aspirin 325 mg and clopidogrel 75 mg daily for his coronary artery stent placed seven days earlier. Computed tomography (CT) angiography of the brain showed severely ectatic left vertebral and basilar arteries consistent with VFA. The right vertebral artery appeared irregular and non-dominant (Fig. 1).
After careful evaluation, endovascular approach was deemed to be the most appropriate treatment. The patient was taken to neurointerventional suite and placed under general anesthesia. A complete 6-vessel cerebral angiogram demonstrated severe dolichoectasia involving the left vertebral and the basilar arteries. It also revealed a 2-mm blister in the right vertebral artery proximal to right PICA take off that was not apparent on pre-operative CT angiogram. Since either the left dolichoectatic vertebrobasilar artery or the right vertebral artery blister aneurysm could be the source of SAH, the decision was made to treat both.
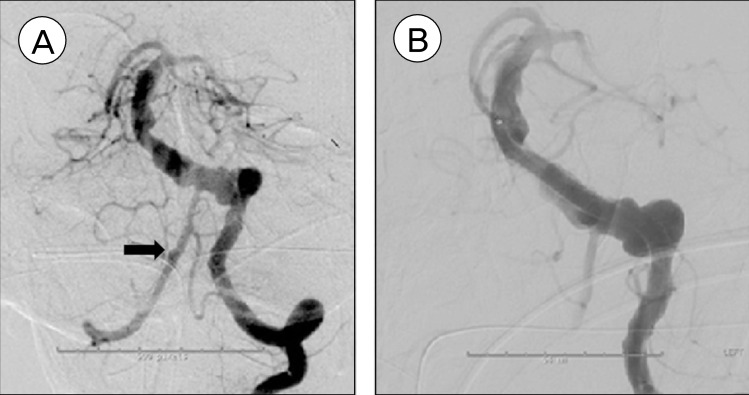
Through a 6 French sheath, a 6F neuron guide catheter (Penumbra, CA) was used to catheterize the left vertebral artery. The patient was given 3,000 units of heparin intravenous injection with an activated clotting time of 214. His aspirin reaction units was 407; clopidogrel activity test showed 73% platelet inhibition with P2Y12 reactivity unit of 98. A Marksman catheter (Covidien, CA) along with a Synchro 2 (Stryker, MI) standard microwire was navigated through the left dolichoectatic vertebral artery into the basilar artery. Next, five PEDs (four 4.5 × 20 mm, one 4.5 × 18 mm) were deployed in a telescoping fashion starting from proximal part of the basilar artery down to the left vertebral artery, essentially reconstructing the entire length of the affected vertebrobasilar system. Each PED was placed within the previous one with 50% overlap. A cerebral angiogram after the PED placement demonstrated good patency of the target vessels and there was stasis in the irregularity outside the PED. Next, the right vertebral artery was selectively catheterized and one additional PED (3.0 × 16 mm) was placed across the blister in the right vertebral artery. The final angiogram from the left vertebral artery demonstrated patency of both vertebral arteries (Fig. 2). No technical complication occurred during the case. The patient was continued on aspirin 325 mg and clopidogrel 75 mg daily.
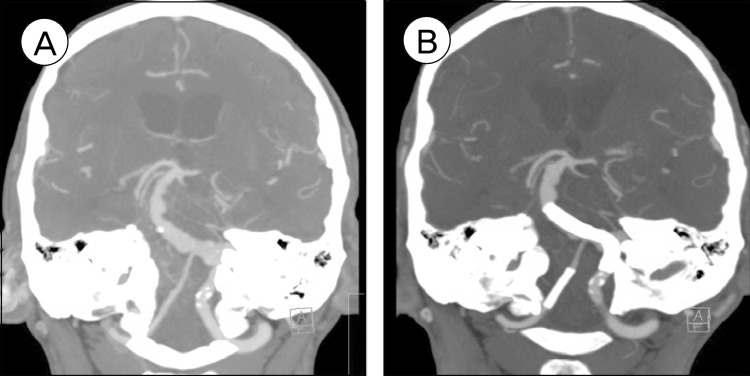
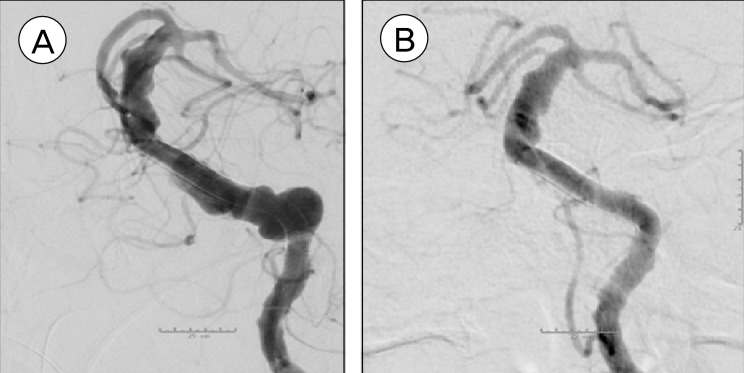
CT angiogram on postoperative day 5 showed patency of the stents (Fig. 3). MRI at three months after the procedure showed no ischemic changes suggesting patency of perforators in the vertebrobasilar system. Conventional cerebral angiogram at six months demonstrated successful reconstruction of the vertebrobasilar system and thrombosis of the VFA (Fig. 4). The patient remained neurologically well and was living independently at home.
DISCUSSION
SAH is an uncommon presentation of VFA and only accounts for about 3.85% of the cases overall.6) However, the risk for re-hemorrhage in these patients is high.4) Open surgical treatment in the setting of SAH in this elderly patient on aspirin and clopidogrel carries high risk. The optimal strategy and treatment goal in this setting would be strengthen and reconstruct the VFA to prevent recurrent hemorrhage and further comprise in vessel wall integrity. The PED is an ideal device in this situation. It provides a metal scaffold for endothelial cells to promote neointimal growth,1-3) which eventually forms an entirely new endothelial-lined lumen with metal reinforced vessel wall. In theory, this would decrease the chance for recurrent hemorrhage and may even deter or halt the disease progression. We recommend not overlapping PED's more than 50% of their length in the posterior circulation to avoid mechanical obstruction of perforators. Ideally, a longer length PED would have been our first choice to allow single device coverage of this aneurysm, but unfortunately, this device is not currently available in the United States.
The drawback of using a stent in the case of acute SAH is that the patient was continued on dual antiplatelet therapy, which might have complicated the hospital course if the patient would have needed external ventricular drainage or a shunting procedure. In addition, the use of PED in the acute phase of SAH is controversial due to the fact that PED might not immediately occlude the area that bled. Other endovascular options would have been sacrifice of the dominant vertebral artery with the hopes that the non-dominant vertebral artery would have sufficient perfusion. However, in this case the non-dominant vertebral artery was diseased as well. The use of regular self-expanding stents would have been an option, but would not have significant flow diversion.
 XML Download
XML Download