

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The importance of ovarian cancer stems not from the fact that it is the sixth most common cancer in women worldwide, but that it is the most lethal gynecologic malignancy in Western Europe and North America, killing more women than uterine and cervical cancer combined. It is predominantly a disease of postmenopausal women with a median age at diagnosis of 60 years.1 Elevated serum cancer antigen 125 (CA-125) levels in postmenopausal women with solid adnexal masses, ascites, and pleural effusion are highly suggestive for malignant ovarian tumor. However, surgery and histological confirmation of the preoperative diagnosis are mandatory, since a minority of patients with these findings have a benign condition, commonly known as Meigs' syndrome This condition disappears after removal of the pelvic tumor.
We report on a case of Meigs' syndrome caused by a left ovarian thecoma with elevated serum CA-125 level in a postmenopausal woman.
Case Report
A 61-year-old Korean woman was admitted to our emergency room because of progressive dyspnea, abdominal distention. Her obstetric history included three uncomplicated deliveries and menopause occurred at the age of 52 years. She had previously been in good health with no medical history and had no family medical history.
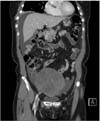
On physical examination, her abdomen was distended with dullness in percussion and a positive shifting dullness. On lung examination, there was a decreased breath sound at the base of the left lung. A chest X-ray showed the presence of a massive right-sided pleural effusion (Fig. 1). On gynecological exam, a pelvic mass was palpated in the left adnexa. Ultrasonography showed a solid mass measuring 12 × 11 cm in the left adnexa with ascitic fluid. Abdominopelvic computed tomography (CT) scan showed a solid heterogeneous mass in the pelvic midline with ascites (Fig. 2). Laboratory investigations showed CA-125 level of 347 IU/mL and other tumor markers were within the normal range. For her dyspnea, she underwent pleural fluid aspiration and cytology showed no malignancy.
Due to clinical suspicion of a malignant ovarian tumor, the patient underwent exploratory laparotomy. During surgery, a lobulated left adnexal solid mass measuring 12 × 11 cm without excrescences was found. The uterus and right adnexa were normal in appearance. Frozen section of the mass was read as benign ovarian thecoma. The liver, bowel, and omentum were grossly free of disease. Postoperative histology confirmed benign thecoma of the left ovary (Fig. 3).
After surgery, all symptoms disappeared and the patient was discharged on the fifth postoperative day. Six weeks postoperatively, she was followed on an outpatient basis without further complaints. During one month after surgery, the pleural effusion was completely resolved on repeat chest X-ray and CA-125 level decreased to 19 IU/mL. The patient was asymptomatic with a normal serum CA-125 level 12 months after the operation.
Discussion
Meigs described the association of pleural effusion and ascites with benign ovarian fibroma.2 Meigs' syndrome includes a pelvic mass or benign ovarian tumor with pleural effusion (hydrothorax) and ascites, which all disappear after tumor removal.3 In menopausal women, detection of any pelvic mass with ascites, hydrothorax, and high serum levels of CA-125 is suggestive of a malignant ovarian tumor. Although it mimics a malignant condition, Meigs' syndrome is a benign disease and has a very good prognosis if properly managed. Life expectancy after surgical removal of the tumor mirrors that of the general population.2 Thecoma is a rare ovarian tumor associated with Meigs' syndrome in just 2% of cases.4
The pathogenesis of the production of ascitic fluid in Meigs' syndrome is uncertain. It has been postulated that the fluid results from an imbalance between vascular supply and lymphatic drainage in these large tumors. An alternate hypothesis is that the process is inflammatory in nature, with an earlier report demonstrating elevations of several inflammatory molecules and cytokines including vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF), interleukin (IL)-1b, IL-6, and IL-8, however, the detailed underlying mechanism is still unclear.5 Interestingly, the preoperative cytokine testing in the patient described in this report showed normal values for IL-1b and IL-8 and only modest elevation of the IL-6 and tumor necrosis factor levels.
The hydrothorax is mainly unilateral and occurs most often on the right-side (75%), rarely the left-side, but can be bilateral. The etiology of pleural effusion is uncertain. It is thought that the occurrence of pleural effusion is secondary to the passage of ascitic fluid to the pleural space through the diaphragm or diaphragmatic lymph vessels, which are more common on the right side.6 The size of the pleural effusion is largely independent of the amount of ascites. The connection between the pelvic tumor and ascites is confirmed by the rapid resolution of abdominal and pleural fluid after removal of the tumor.
The elevation of the tumor marker CA-125 is a confounding factor in that CA-125 is increased in 80% of epithelial ovarian cancers but also in other malignancies and benign tumors.7 CA-125 antigen is a glycoprotein with a high molecular weight is recognized by a monoclonal antibody. It is expressed in the amnion and embryonic coelomic epithelium.8 The antigen can also appear in many adult tissues, including the epithelium of fallopian tubes, endometrium, endocervix, and ovaries.9 In addition, it is found in mesothelial cells of the pleura, pericardium, and peritoneum. Therefore, some normal body tissues can produce a certain and low level of circulatory or serum CA-125. This tumor marker is elevated during menstruation or pregnancy and in some benign conditions such as endometriosis, peritonitis or cirrhosis, particularly with ascites.10,11 It is also increased in vascular invasion, tissue destruction and inflammation associated with malignant disease. In a series by O'Connell et al.,12 the predictive value of a CA-125 level greater than 35 U/mL was 60% for ovarian cancer and 84% for some types of malignancy. The authors also reported on three patients with ovarian fibroma and elevated serum CA-125 levels (above 35 U/mL) in their series.
Postmenopausal women with clinical conditions of palpable pelvic masses, ascites, pleural effusion, and elevated serum CA-125 levels probably have malignant ovarian tumors. However, etiology of thecoma forming part of Meigs' syndrome is benign even in the presence of an elevated serum CA-125 level.


 XML Download
XML Download