

 PDF
PDF ePub
ePub Citation
Citation Print
Print



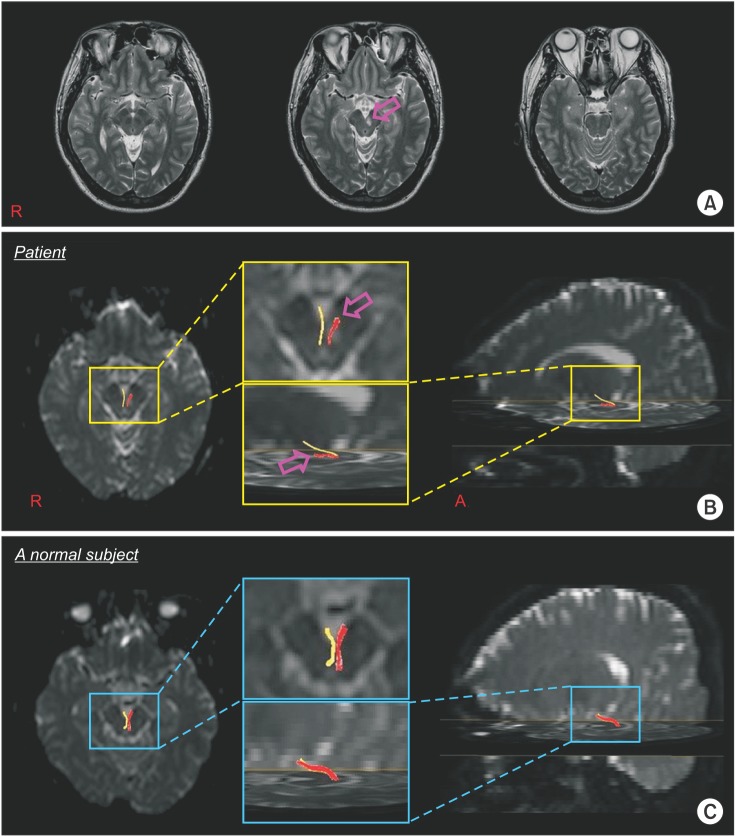
A 39-year-old male patient, diagnosed with a cerebral infarct in the left midbrain, visited Yeungnam University Hospital and underwent conservative management. Brain magnetic resonance imaging performed at 1 week from onset showed a leukomalactic lesion in the left midbrain (Fig. 1A). Mild ptosis (3 mm) and mild limitation in the upward (20°) and medical (10°) gaze were observed. However, his left eye was not deviated, and did not show mydriasis.
Diffusion tensor imaging (DTI) data were acquired one week after onset. A 6-channel head coil on a 1.5T Philips Gyroscan Intera (Philips, Best, The Netherlands) with single-shot echo-planar imaging was used for scanning. DTI-Studio software was used for the reconstruction of the oculomotor nerve. Fibers passing through two regions of interest (ROIs) were depicted with a fractional anisotropy of >0.2 and a tract turning-angle of <60°. Following the known anatomy, the first ROI was given at the periaqueductal region, and the second one at the oculomotor nerve area of the ventral part of the midbrain, with an option of cut operation on the axial images [12345].
Diffusion tensor tractography (DTT) revealed a discontinuation of the left oculomotor nerve in the area where the nerve exited the left midbrain (Fig. 1B). This patient showed mild ptosis and limitations of eye movement in his left eye; these mild dysfunctions appeared to result from the injured left oculomotor nerve, caused by the left midbrain infarct. Our results suggest that DTT is useful to demonstrate injury to the oculomotor nerve for patients with clinical features of oculomotor nerve palsy after cerebral infarct [12345].
 XML Download
XML Download