

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Common fibular neuropathy (CFN) is the most frequent mononeuropathy in the lower extremity [1]. The common fibular nerve, split from sciatic nerve, runs through the popliteal fossa laterally and curves distally around the fibular head (FH) and then divides into superficial and deep branches. The FH is the most common site of lesion in CFN [2]. Main causes of CFN at this level are external compression or direct trauma. Ganglion and systemic disorders such as diabetes mellitus or alcoholism are also known to cause neuropathy [134]. Clinically, patients with CFN at the FH mainly present with foot drop due to weakness of ankle dorsiflexion and paresthesia over lateral calf and dorsum of the foot. However, these symptoms may also be seen in other clinical conditions, including sciatic mononeuropathy, lumbosacral plexopathy, or lumbar radiculopathy [14]. Therefore, accurate diagnosis and identification of etiology should be made through thorough and straightforward diagnostic measurement. Traditionally, electrophysiologic study has been considered a mainstay in diagnosing peripheral nerve disorder, including CFN at the FH [45]. Alternatively, ultrasonography a noninvasive means for high-resolution dynamic images in real time has become a preferred tool for assessing peripheral nerves, compensating the limitations of electrophysiologic study such as invasiveness [156]. In addition, ultrasonography shows higher sensitivity, as compared to MRI in noninvasive diagnosis of nerve disorders. The sensitivity of ultrasonography is reportedly 93%, as compared to 67% for MRI, with similar specificity (86%) [7].
Nerve enlargement on ultrasonographic measurementis a significant finding in nerve disorders. Measurement of cross-sectional area (CSA) of the nerve is the most widely accepted and reliable method for the diagnosis of nerve disorders [68910]. Thus, determination of reference value of CSA is crucial to identification of nerve pathology and proper diagnosis [69]. However, there are few systemic studies and no standard consensus on ultrasonographic measurements and diagnostic cutoff value for the CFN at the FH [169101112]. Several studies reported ultrasonographic findings of patients with foot drop and demonstrated the value of ultrasonography as a diagnostic tool; however, they included small number of patients [11112]. Moreover, one of the studies on subjects whose etiology was confined to weight loss showed no significant difference in nerve thickening between symptomatic and asymptomatic sides [12]. Recently, >8 mm2 was determined as cutoff value of CF nerve CSA at the FH with a sensitivity of 86% and a specificity of 73%. Although it was the first report in literature that suggested cutoff value of CF nerve CSA at the FH, the specificity was somewhat low; and there was no comparison of symptomatic and asymptomatic side or that of affected site and nonaffected site at symptomatic side. Also, the 9 subjects with neuropathy other than CFN showed even larger CF nerve at the FH, as compared to healthy controls, contrary to general expectation [10]. As compared to previous studies, greater number of patients with CFN at the FH with no biased distribution of etiology were included in this study. In addition to absolute nerve CSA, swelling ratio and comparison of symptomatic side and asymptomatic side were also analyzed. Therefore, this study aimed to establish the diagnostic cutoff value of the ultrasonographic measurements, and verify its diagnostic usefulness and efficacy for CFN at the FH.
MATERIALS AND METHODS
Medical records of 20 patients who visited Yeouido St. Mary's Hospital from January 2013 to April 2014 were reviewed retrospectively; and a control group of 30 healthy age-matched asymptomatic adults were recruited. Ultrasonographic records of right legs were examined prospectively. The study was approved by the Institutional Review Board of Yeouido St. Mary's Hospital. Twenty patients with confirmed CFN at the FH by electrodiagnostic study were included in the patient group. Patients with previous history of trauma or lower leg surgery were excluded. Patients with neurologic disease other than CFN, such as central nervous system disorder, polyneuropathy or combined lumbosacral radiculopathy, plexopathy and sciatic neuropathy were also excluded from the study. Electrodiagnosis was based on recommended guidelines by Preston and Shapiro [13]: (1) slow motor conduction across the FH (delay in the nerve conduction velocity of >10 m/s across the FH), (2) conduction block across the FH (a drop in compound muscle action potential amplitude of >20%), (3) delay of peak latency or a decrease in amplitude in superficial peroneal nerve, and (4) needle electromyograghic abnormalities in at least one peroneal-innervated muscle. Diagnosis of CFN at the FH was confirmed if either (1) or (2) with definite (3), where (4) is considered as an accessory finding [14]. Nerve conduction studies and electromyographic finding of the other nerves, except CF nerve, were required to be normal [10].
Ultrasonography was performed by a physiatrist blinded to the results of clinical and electrodiagnostic study, using a Voluson E ultrasound device (GE Healthcare, Waukesha, WI, USA) with a 7–12 MHz linear–array transducer. The physiatrist had more than 3 years of musculoskeletal ultrasonography experience and performed ultrasonography in the outpatient clinic on a daily basis. The probe was carefully placed perpendicular to the nerve to minimize anisotropy and no additional force was applied other than the weight of probe. On transverse scans, the full course of the CF nerve was assessed from the PF to the lateral aspect of the FH, and CSA was measured by continuously tracing inside of hyperechoic epineural rim of the nerve (Fig. 1). During evaluation, both patients and controls were placed in the prone position with knees fully extended. CSA measurements were repeated thrice consecutively and the mean values were obtained. Intra-rater correlation coefficients calculated from control group showed good reliability (>0.8).
CSA was measured at 3 anatomic levels in both groups, as follows: (1) sciatic nerve at mid-thigh level at the site of midpoint of gluteal fold and popliteal crease, (2) CF nerve at the PF just distal to the point of bifurcation from sciatic nerve, and (3) CF nerve at the level of FH before the fibular tunnel. At this site, the largest CSA was recorded.
In order to improve accuracy of the ultrasonographic measurement of CFN at the FH [10], in addition to CSA, the following values were calculated: (1) the difference of CF nerve CSA at the FH between symptomatic side and asymptomatic side (ΔSx–Asx) (2) the ratio of CF nerve CSA at the FH to at the PF (FH/PF) (3) the ratio of CF nerve CSA at the FH symptomatic side to asymptomatic side (Ratio Sx–Asx). In control group, ΔSx–Asx and Ratio Sx–Asx were obtained from CSA at the FH of right and left sides.
Statistical analysis
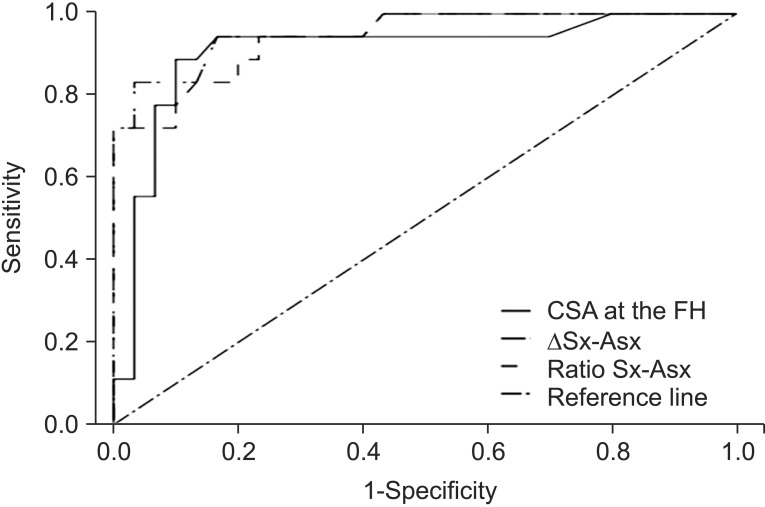
Statistical analysis was performed with SPSS ver. 17 for Windows (SPSS Inc., Chicago, IL, USA). The chi-square test was used to compare the baseline characteristics of the patients and control groups. The Mann-Whitney U-test was used to analyze differences in CSA measurements and their ratios between the two groups. Threshold of significance was defined as p<0.05, in all tests. A receiver operating characteristic (ROC) analysis was performed to determine optimal cutoff values of the ultrasonographic measurements in diagnosing CFN at the FH, and specificity and sensitivity were obtained.
RESULTS
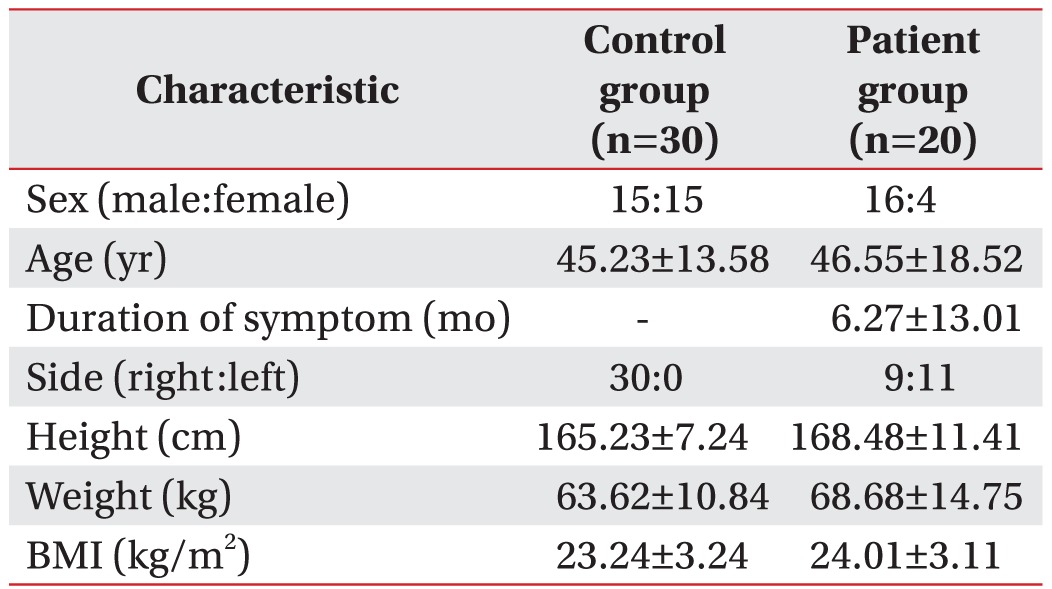
A total of 20 patients and 30 healthy controls were studied. The baseline characteristics showed no significant differences between the two groups (p>0.05) (Table 1).
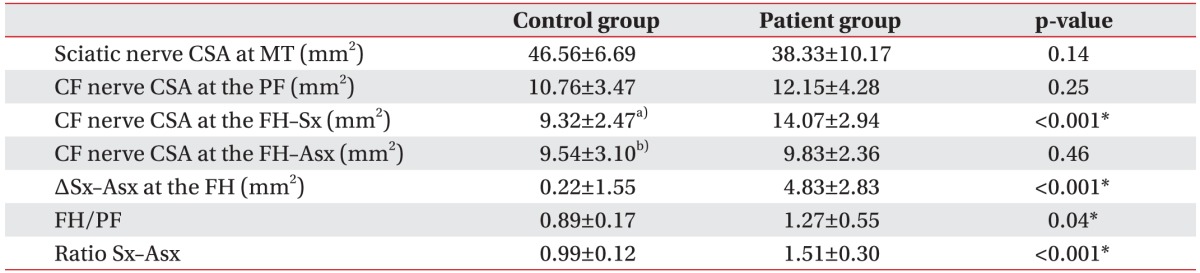
Nerve CSA were measured at 3 anatomic levels, as described in Table 2. In patients group, the mean CF nerve CSA at the FH was 14.07±2.94 mm2 and the difference of CF nerve CSA at the FH between symptomatic side and asymptomatic side (ΔSx–Asx) was 4.83±2.83 mm2, with significant difference, as compared to control groups (p<0.001 for all). As expected, the mean CSA of sciatic nerve at mid-thigh and that of CF nerve at the PF showed no significant differences between the two groups (p=0.14 and p=0.25, respectively).
In addition, the FH/PF (1.27±0.55) and the Ratio Sx–Asx (1.51±0.30) were significantly larger than that of control group (p=0.04 and p<0.001, respectively) (Table 2).
The diagnostic sensitivity and specificity of ultrasonographic measurements and their ratios were compared by ROC analysis. The cutoff value for the diagnosis of CFN at the FH was 11.70 mm2 for the CF nerve CSA at the FH (sensitivity 85.0%, specificity 90.0%), 1.7 mm2 for the ΔSx–Asx (sensitivity 83.3%, specificity 96.7%), 1.11 for the FH/PF (sensitivity 47.1%, specificity 72.2%), and 1.24 for the Ratio Sx-Asx (sensitivity 72.2%, specificity 96.7%), respectively. The ΔSx–Asx had the largest area under the curve (AUC, 0.96) (Table 3, Fig. 2).
DISCUSSION
To date, many studies have reported that ultrasonographic measurement is a beneficial diagnostic tool for nerve disorders with significant positive correlation with electrodiagnostic study [111516171819]. Ultrasonography visualizes the anatomy of the affected structures and provides morphological information. In some cases, it is crucial for developing therapeutic plans and determining prognosis. In case of CFN at the FH secondary to the intraneural ganglion cyst that needs surgical procedure, ultrasonography leads to more accurate prognosis by detecting the etiology, which might not be identified by electrophysiological study alone [15]. Moreover, if electrodiagnostic study is performed inadequately or insufficiently, ultrasonography could be a supplementary tool for accurate diagnosis by differentiating from lesions that mimic CFN at the FH such as high sciatic nerve lesion [11]. Ultrasonography in addition to electrodiagnostic study reportedly improves specificity to 88% in CFN at the FH [10] and sensitivity up to 98% in ulnar neuropathy at the elbow [18].
In this study, by conducting ultrasonographic measurement on patients with electrodiagnostically diagnosed CFN at the FH, several cutoff values were confirmed for statistical significance in diagnosing neuropathy.
At the FH, patients had significantly larger mean CSA of CF nerve than controls, consistent with previous studies [101112]; and cutoff value by the ROC curve was 11.7 mm2, with a sensitivity of 85.0% and specificity of 90.0%. Mean CSA was 14.07 mm2, which is larger than 10.9 mm2 reported by Visser et al. [10], but smaller than 17.9 mm2 reported by Cruz-Martinez et al. [12], and 26.2 mm2 reported by Lo et al. [11]. Thus, the reported mean CSA had a wide distribution from 11 mm2 to 18 mm2, possibly due to different demographic factors such as height or weight and inclusion of normal healthy subjects alone [610122021].
To overcome these discrepancies, in clinical practice, the healthy contralateral side is often used as an internal control [222324]. Some previous studies described upper limit value of the side-to-side difference [6922]; in addition, one study showed no significant correlation with subjects' baseline demographic factors including age, height, weight, and BMI in CF nerve [9]. Therefore, these absolute values could be a useful reference for detection of nerve pathology in people with different age and body index [691022]. In our study, mean value of ΔSx–Asx was 4.83±2.83 mm2 and ΔSx–Asx of 1.7 mm2 as cutoff value yielded a sensitivity of 83.3% and a specificity 96.7%. In agreement with our findings, previous studies reported 3.2 mm2 and 4.9 mm2 upper limit of side-to-side difference, respectively; but data were obtained from healthy subjects and the validity or diagnostic accuracy were not assessed [69].
Although ΔSx–Asx was a useful and reliable value, it is not applicable to bilateral lesions or diffuse nerve pathology [222324]. Therefore, the ratio of nerve CSA has also been analyzed and proposed as a complementary value [252627]. The swelling ratio of CSA between affected site and unaffected sites is a beneficial method, but most studies are limited to upper extremity nerve disorders, such as carpal tunnel syndrome and ulnar neuropathy at the elbow [16232526]. In this study, ratio Sx–Asx had sensitivity (72.2%) and specificity (96.7%) at >1.24 cutoff value. This value could be helpful, especially in differentiating focal nerve swelling from more diffuse nerve enlargement, such as existing polyneuropathy, which may be due to diabetes mellitus or alcoholism [10252728].
This study had the limitation of a relatively small number of participants. However, the number of participants in our study exceeded that of previous studies and subjects in patients group had wide variety of etiologies including trauma (30%), prolonged position or compression (25%), space occupying lesion around FH (10%), and metabolic disorders (10%). Therefore, the result of this study could be used as a generalized standard for patients with CPN at the FH and is considered as representative [123411].
In conclusion, ultrasonographic evaluation of CF nerve and CSA measurement is a helpful and complementary tool for diagnosing CFN at the FH. The diagnostic cutoff value of the ultrasonographic measurements was established and efficacy and validity were verified. Furthermore, this investigation is the first to demonstrate ratio of nerve CSA as useful values, minimizing the effect of demographic factors such as height and BMI. These diagnostic values could facilitate accurate and proper diagnosis of CFN at the FH in clinical practice.


 XML Download
XML Download