

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Benign prostatic hyperplasia (BPH) is the main reason for lower urinary tract symptoms (LUTS) due to urethral blockade [1]. There are two kinds of treatments for patients with BPH: medical treatment and surgical treatment [2]. Medical treatment using alpha-blockers or/and 5-alpha reductase inhibitors (5α-RIs) is the first-line treatment for BPH [3]. Finasteride is a type II and type III 5α-RIs [4]. Finasteride 5 mg is used to treat symptomatic BPH to shrink the prostate and reduce the risk of urinary retention caused by restricted urine flow when prostate becomes enlarged. Improving symptoms of BPH with finasteride 5 mg also reduces the need for surgery.
Finasteride is also approved for treating male androgenetic alopecia (MAA) at low dose. Dihydrotestosterone (DHT) is thought to play a significant role in inducing MAA. It is formed from the conversion of circulating testosterone to DHT by 5-alpha reductase (5α-R) [5]. There are three known isoenzymes of 5α-R receptors. Type I and type II 5α-R play an important role in the treatment of MAA [6]. Type I 5α-R is predominantly located in the skin, including sebaceous glands and hair follicles. Type II 5α-R is the major contributor to DHT pool. It is located in the inner root sheath of hair follicles in the scalp, beard, and chest as well as genitals and prostate gland. Type II 5α-RIs such as finasteride are commonly used to stabilize hair loss and promote regrowth.
Although BPH itself is an independent risk factor for erectile dysfunction (ED), evidence suggests that 5α-RIs such as finasteride may independently increase the risk of adverse sexual side effects potentially through inducing androgen deficiency by inhibiting 5α-R and reducing available 5α-DHT [78]. Actually, patients with BPH who used finasteride to treat their disease experienced worsening erectile function (EF) that did not resolve with continued treatment, although some studies reported that continuous treatment with finasteride decreased ED [8]. These sexual side effects are persistent or irreversible in some patients. The importance of 5α-DHT in development and maintenance of male sexual organs and its function have been noted in several studies [910]. However, many investigators believe that side effects of 5α-RIs will disappear with continuous treatment. Furthermore, side effects of 5α-RIs on EF have received minimal attention and deemed clinically less important [781112]. Considerable controversy exists regarding the severity and persistence of side effects of finasteride. Therefore, the aim of this review was to summarize current research studies on finasteride associated with ED.
PATHOPHYSIOLOGY OF FINASTERIDE AND ERECTILE DYSFUNCTION
Androgen plays an essential role in maintaining the structure and function of the penis. However, finasteride is an competitive inhibitor of type II 5α-R [13]. Finasteride is developed to decrease the conversion of testosterone to its more potent metabolite 5α-DHT. Based on literatures, finasteride can achieve 70–80% reduction in DHT [13]. Traish et al [14] have found that castration can decrease smooth muscle components and increase collagen tissue in the corpus cavernosum. Zhang et al [15] have reported that prolonged administration of 5α-RIs in aged rats can attenuate erectile response to electrical stimulation of the cavernous nerve. Mechanisms responsible for such effects could be due to structural changes, decreased autophagy, aggravated ultrastructural injury of mitochondria, and increased apoptosis, of the smooth muscle cells of the 5α-RIs-treatment rat group [15].
Some clinical studies already showed that the 5α-RIs treatment caused the increase of serum testosterone levels. Roehrborn et al [16] reported that finasteride treatment led to a significant increase relative to placebo in serum testosterone. Also, Hong et al [17] reported that dutasteride treatment in men with BPH led to a significant increase in serum testosterone levels. Despite the increase of total testosterone after finasteride treatment, ED is more influenced by the decrease of DHT. Because, DHT has higher affinity for the androgen receptors and more effective at increasing nitric oxide (NO) synthase expression than total testosterone [1819].
EF is perceived in the brain where receptors for testosterones are widely distributed. 5α-R activity is also found in neurons, oligodendrocytes, and astrocytes [20]. Neuronal and glial cell development may be promoted by androgens metabolized by 5α-R [21]. Finasteride can cross the blood-brain barrier and inhibit the production of DHT throughout the central nervous system [22]. It is biologically plausible that a lack of DHT or another 5α-reduced hormone is responsible for a decrease in libido resulting in ED [23]. Because pathogenesis of ED is multifactorial and involve psychogenic and organic components [24], decrease of the libido caused by finasteride can contribute to the development of ED.
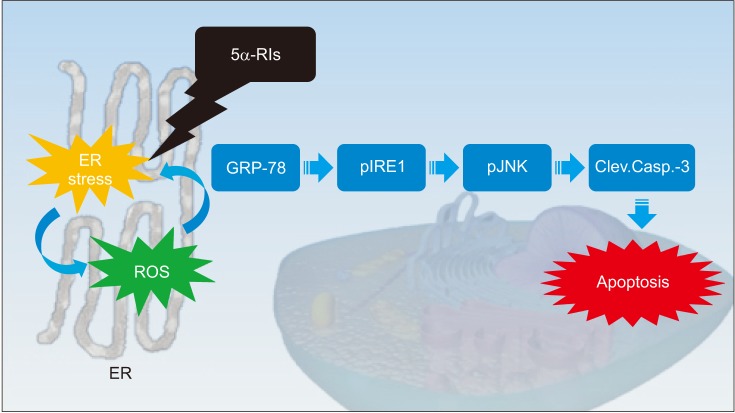
We investigated the ability of reactive oxygen species ROS) to evoke endoplasmic reticulum (ER) stress in a finasteride animal model and found that the unfolded protein response (UPR) effectors (glucose-regulated protein-78, phosphorylated c-jun-N-terminal kinase and phosphorylated inositol-requiring transmembrane kinase/endoribonuclease) and apoptotic markers (procaspase-3 and cleaved caspase-3) were triggered in a ROS-dependent manner (Fig. 1) [25]. The overproduction of ROS induce a decrease in the bioavailability of NO in the corpus cavernosum, impairing vascular smooth muscle relaxation through the NO-cyclic guanosine monophosphate pathway [2627]. ROS interfere with the folding process of polypeptides in the ER, therefore ER stress appears to damage vascular endothelial cells and compromise vascular relaxation of the corpus cavernosum [28]. In our opinion, ER stress caused by finasteride could be a mechanism of leading to ED. In addition to basic research, a large and randomized prospective clinical studies should be required to clarify these findings.
RECENT RESEARCH OF FINASTERIDE FOR BENIGN PROSTATIC HYPERPLASIA AND ERECTILE DYSFUNCTION
Most studies in this review have revealed that finasteride for BPH is correlated with ED. A summary of findings discussed below is presented in Table 1.
Recently, Corona et al [29] have conducted a comprehensive review and meta-analysis for ED in subjects treated with 5α-RIs, including finasteride for BPH. An extensive Medline Embase and Cochrane search was performed including the following words: ‘finasteride’, ‘dutasteride’, and ‘benign prostatic hyperplasia’. Only placebo-controlled randomized clinical trials evaluating the effect of 5α-RIs in subjects with BPH were considered. Of 383 retrieved articles, 17 were included in this study. Randomized clinical trials enrolled 24,463 in the active arm and 22,270 patients in the placebo arm, with a mean follow-up of 99 weeks and a mean age of 64.0 years. Overall, 5α-RIs increased the risk of hypoactive sexual desire (odds ratio [OR]=1.54; 95% confidence interval [CI], 1.29–1.82; p<0.0001) and ED (OR=1.47; 95% CI, 1.29–1.68; p<0.0001). Their data showed that the use of 5α-RIs significantly increased the risk of ED, ejaculatory dysfunction, and hypoactive sexual desire in subjects with BPH.
In 2016, Liu et al [30] reported a meta-analysis and systematic review of randomized controlled trials for ED in subjects treated with 5α-RIs, including finasteride for BPH. Their study included 10 trials (6,779 patients) on the efficacy and safety of finasteride 5 mg for BPH. The mean age of participants was 60.10 years across all studies. Pooled relative risk for sexual dysfunction was 2.56 (95% confidence interval [CI]=1.48–4.42) and that for ED was 1.55 (95% CI=1.14–2.12) in men with BPH. Sexual function also worsened with time in the 5α-RIs groups. These findings suggested that 5α-RIs were associated with 156% increased risk of sexual dysfunction for men with BPH. Furthermore, therapy lasting at least 1 year was associated with a statistically significant increased risk of adverse sexual effects compared with placebo (p=0.047 and p=0.002, respectively). Their study, the largest meta-analysis to date on the effect of 5α-RIs on sexual function, demonstrated that 5α-RIs are associated with a significantly higher risk of ED than placebo in men with BPH.
However, other studies have presented different results. Results of a study published in 2016 have provided evidence that 5α-RIs do not increase the risk of clinically meaningful incident ED in men who are free of sexual dysfunction, regardless of indication for use for BPH [31]. In the population with BPH (aged 40 years or more) (n=71,849), the risk of ED was not increased with use of 5α-RIs only (incidence rate ratio: 0.92, 95% CI: 0.85–0.99; OR: 0.94, 95% CI: 0.85–1.03) or 5α-RIs+α blocker (incidence rate ratio: 1.09, 95% CI: 0.99–1.21; OR: 0.92, 95% CI: 0.80–1.06) compared to the use of α blockers only. The risk remained null regardless of the number of prescriptions or timing of use. There were no proven causal connections between 5a-RIs and symptoms of sexual dysfunction reported by patients.
In 2015, Traish et al [32] reported that long-term finasteride therapy results in worsening of EF and lower total testosterone levels in men with BPH. In their retrospective registry study, a cohort of 470 men aged between 47 and 68 years (mean: 57.78±4.81 years) were treated with finasteride 5 mg. A second cohort of 230 men aged between 52 and 72 years (mean: 62.62±4.65 years) were treated with tamsulosin 0.4 mg. All men were followed-up for 45 months. At intervals of 3 months, plasma testosterone levels and International Index of Erectile Function (IIEF)-EF questionnaire scores were determined at each visit. Long-term treatment with finasteride therapy was associated with worsening of ED as shown by significant decrease in IIEF-EF scores in men treated with finasteride. The increase in ED due to finasteride was not resolved by continuing the treatment with finasteride. Most importantly, long-term finasteride therapy resulted in reduced total testosterone levels that contributed to a state of hypogonadism [32].
In MTOPS (Medical Therapy of Prostatic Symptoms) study, a multicenter, randomized, double-blind, placebo controlled clinical trial was performed with time to BPH progression as the primary outcome and change in sexual function as the secondary outcome [33]. They analyzed records of 2,783 men who completed the inventory at baseline and at least once during follow-up [33]. These men had an average age of 62.6±7.3 years. Treatment with finasteride or finasteride combined therapy with doxazosin was associated with worsening sexual function compared to placebo. There was no significant difference in changes in sexual function in men assigned to doxazosin alone compared to placebo.
In 2012, Zhang et al [34] reported that finasteride treatment for 4 weeks reduced the weight of the corpus cavernosum without appearing to affect erectile responses to electrical stimulation of the cavernous nerve in a rat model. Adult male Sprague-Dawley rats were divided into four groups (n=25/group): (i) control; (ii) castration; (iii) castration with testosterone replacement; and (iv) oral finasteride treatment. Four weeks later, erectile function was measured by the ratio of intracavernosal pressure and mean arterial blood pressure upon electrical stimulation of the cavernous nerve. Tissue weights of the corpus cavernosum and prostate were reduced by 25.9% and 92.3% in group 4 compared to those in group 1 (both p<0.001). However, there was no significant difference in serum testosterone concentration or erectile function between groups 4 and 1. The author's explain that as erection is a complex process involving important signaling in the brain, further studies are necessary to demonstrate the long-term effects of finasteride on both central and peripheral neural pathways of erection. However, nobody knows that the erectile response to electrical field stimulation may be different comparing with normal physiologic EF in threshold to stimulation.
RECENT RESEARCH OF FINASTERIDE FOR MALE ANDROGENETIC ALOPECIA AND ERECTILE DYSFUNCTION
Most studies included in this review revealed that finasteride for MAA was not correlated with ED. A summary of findings discussed below is presented in Table 2.
Recently, Liu et al [30] reported a meta-analysis and a systematic review of randomized controlled trials for ED in subjects treated with 5α-RIs, including finasteride for MAA. Their study included three trials (4,493 patients) on the efficacy and safety of finasteride and dutasteride for MAA. The mean age of participants was 60.10 years across all studies. Pooled relative risk for sexual dysfunction was 1.21 (95% CI: 0.85–1.72) and that for ED was 0.66 (95% CI: 0.20–2.25) in men with MAA. Also, there was no significant association between duration of therapy and adverse sexual effects in men with MAA. Evidence from these randomized controlled trials suggested that the association between finasteride and ED was not statistically significant in men with MAA.
Hagberg et al [31] have conducted a cohort study using Clinical Practice Research Datalink for ED in subjects treated with 5α-RIs, including finasteride for MAA. For the MAA population (aged 18–59 years) (n=12,346), the risk of ED was not increased for users of finasteride 1 mg compared to unexposed men with MAA (incidence rate ratio: 1.03, 95% CI: 0.73–1.44; OR: 0.95, 95% CI: 0.64–1.41).
However, other studies have revealed different results. In 2016, Chiriacò et al [35] showed that finasteride therapy for MAA resulted in worsening of ED. In their retrospective registry study, among 79 participants, 34% were white Italians with mean age of 33.4±7.60 years, mean duration of finasteride use of 27.3±33.21 months, and mean time from finasteride discontinuation of 44.1±34.20 months. Symptoms were investigated by an ad hoc 100 questions' questionnaire and validated Arizona Sexual Experience Scale and Aging Male Symptom Scale questionnaires. By validated Arizona Sexual Experience Scale questionnaire, 40.5% of participants declared that getting and keeping erection were very difficult while 3.8% of participants never achieved erection. Reaching orgasm was declared to be very difficult by 16.5% of participants and never achieved was declared by 2.5% of participants. By the ad hoc questionnaire, the most frequent sexual symptoms referred were loss of penis sensitivity (87.3%), decreased ejaculatory force (82.3%), and low penile temperature (78.5%). In their study, unexpectedly loss of penis sensitivity was more frequent than severe ED while loss of muscle tone/mass was affecting half of these subjects.
In 2015, Narasimhalu [36] reported results of randomized controlled trials for ED in subjects treated with finasteride for MAA. A questionnaire based on the IIEF was given to approximately 586 patients with MAA who were being treated with finasteride 1 mg for an average of 16 weeks. Statistical analysis of results showed no significant difference in scores between patients taking finasteride and those in the control group. This study suggested that ED was not a side effect of finasteride. In addition, 16 weeks with finasteride 1 mg did not have enough dosage to result in symptomatic ED because patients with MAA were too young in age to have ED.
COMMENTS
Although there is not enough evidence to prove the relationship between finasteride and ED, the nocebo effect should be taken into account when studying sexual effects of finasteride [37]. Most studies in this review found that finasteride for BPH was correlated with ED whereas finasteride for MAA was not correlated with ED.
In our opinion, such difference in outcome might be due to different doses of BPH and MAA treatment with finasteride. Related studies have reported a lower occurrence of sexual adverse events with lower dose of finasteride [3738]. This suggests that different risks of ED between the two groups (finasteride for BPH and finasteride for MAA) might be related to dosage of finasteride.
And the most important factor is difference of age in BPH and MAA patients. BPH patients were much older than MAA patients who participated in these clinical studies. Several studies have reported that the prevalence of ED is 2% to 9% in the decades from 40 to 49 years and 20% to 40% for men aged <69 years. However, the prevalence in men in their 70s and 80s is much higher [39]. The ageing process is accompanied by a progressively increasing of organic impairment. Therefore, the more the global population ages, the more they are affected by several comorbidities [40414243444546]. In elderly patients, finasteride seems to have more adverse effects on sexual dysfunction such as ED.
Data from epidemiological studies suggest a link between symptoms of BPH and ED in older men regardless of age, co-morbidity, or lifestyle [47484950]. Possible connection between these two diseases lies in the mechanism of action of α-1 adrenergic receptor. These receptors might increase the tone of smooth muscle cells of the prostatic capsule and bladder neck in these patients. Penile erection depends on a balanced contraction and relaxation of the cavernous smooth muscle [51]. In ED, the aforementioned receptors affect noradrenaline and androgens and favor the contraction of smooth muscle. This may complicate the process of relaxation of the same muscle and lead to ED [52]. In BPH compared to MAA, the correlation between BPH and ED seems to have more influence than the adverse effect of finasteride on ED.
Although most studies in this review found that finasteride for MAA was not correlated with ED, some patients reported side effects of finasteride associated with sexual dysfunction, including ED, male infertility, and loss of libido [85354555657]. Di Loreto et al [58] have suggested a mechanism of relationship between ED and finasteride in MAA patients. Androgen receptor and nerve density in foreskin prepuce specimens are associated with persistent sexual side effects, including loss of sensitivity in the genital area due to former finasteride use against MAA. In their study, 8 males (aged 29–43 years) reported ED, including loss of penis sensitivity over 6 months after discontinuation of finasteride. Controls were 11 otherwise healthy matched men (aged 23–49 years) who had undergone circumcision for phimosis. They never took finasteride or analogues. Differences in androgen receptor expression and nerve density in different portions of dermal prepuce were evaluated in these two groups. Density of nuclear androgen receptor in stromal and epithelial cells was found to be higher in cases (mean 40.0%, and 80.6% of positive cells, respectively) than that in controls (mean 23.4%, and 65.0% of positive cells, respectively) (p=0.023 and p=0.043, respectively). This provides the first evidence of molecular and objective difference between patients with long-term adverse sexual effects after finasteride use vs. drug untreated healthy controls in certain tissues.
ED induced by finasteride might be due to ER stress. In the present study, Finasteride resulted in reduced fertility and increased ER stress and apoptotic markers in the SD rats [25]. Sperm damage occurs when oxidative stress overcomes natural antioxidant defenses. Accumulation of free radicals coupled with an increase in oxidative stress has been implicated in the pathogenesis of several disease states. Oxidative stress is a crucial regulator of ER function and activation of the UPR in disease conditions, as ER stress and increased oxidative stress production occur concurrently [262728]. Oxidative stress can lead to ED by endothelial dysfunction in part through the activation of ER stress. Therefore, the mechanism of ED associated with finasteride needs to be clarified in the future.
Finally, we have to worry about the unexpected occurrences of 5α-RIs inducing sexual problems during the treatment in young patients who didn't have sexual problems before the treatment [23]. In the aged BPH patients who had been treated with 5α-RIs, they frequently complained the decrease in ejaculation volume and of libido. Similarly, when a young patient who has MAA and is treated with the 5α-RIs treatment, the patient could also complain the same side effects. Furthermore, it should be noted that patients might not be able to recover from the sexual problems even after the discontinuation of the 5α-RIs, and as a result might significantly deteriorate their quality of life. Therefore, physicians should discuss with their patients the possible long-term effect of finasteride on sexual function, even in MAA patients.
CONCLUSION
We reviewed most recent studies of finasteride treatment for BPH and MAA and the occurrence of ED. Evidence from clinical studies suggested that finasteride was associated with increased adverse effects on ED in men with BPH. However, such association was not statistically significant in men with MAA. Some studies reported that finasteride had side effects on sexual dysfunction, including ED, male infertility, ejaculatory dysfunction, and loss of libido, even in MAA patients. Therefore, well-designed randomized controlled trials are needed to determine the mechanism and effects of finasteride on ED. Physicians needs to discuss the possible long-term effect of finasteride ED with their patients, especially in the young healthy patients.


 XML Download
XML Download