

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Müllerian anomalies are frequently associated with renal and skeletal abnormalities but exist in functioning ovaries and normal external genitalia [1]. The prevalence of Müllerian anomalies varies depending on the population studied; the prevalence in the general population ranges from 0.5% to 5.5% [1]. Uterus didelphys accounts for approximately 11% of congenital uterine anomalies [1] and is associated with a single fallopian tube, ovarian malposition, and renal agenesis [2]. Müllerian anomalies with gynecologic malignancies are very rare, and only a few cases have been reported [3], one of which is endometrial cancer associated with uterus didelphys. There are no recorded cases of ovarian malignancies associated with Müllerian anomalies. Herein, we present a case of dysgerminoma with uterus didelphys and right renal agenesis.
Case report
A 34-year-old woman (gravida 0, para 0) was admitted to Busan Paik Hospital owing to abdominal pain and secondary amenorrhea with ovarian mass and uterine anomaly. History of the patient revealed that menarche was at 13 years of age and that her menstrual cycle was regular at 30-day intervals, until 2 years ago. Ovarian mass and uterine anomaly were discovered on transvaginal ultrasound during examination for amenorrhea and abdominal pain at a local clinic. She had been on medications for hypertension and hypothyroidism for one year. On pelvic examination, normal cervix and vagina were noted. Transvaginal ultrasound showed a 9×8-cm septated mass with mixed echogenicity in the right ovary. Uterus didelphys was seen; however, the left ovary was invisible. Abdominal and pelvic computed tomography (APCT) revealed a 10-cm right ovarian tumor with internal necrosis; the mass was suspected to be tubo-ovarian abscess (Fig. 1A), and uterus didelphys, right renal agenesis, left lower ureteral stricture, and left hydronephroureterosis were observed (Fig. 1B). The initial serum CA-125 level was 44.91 U/mL; lactic dehydrogenase level, 274 U/L; anti-Müllerian hormone level, <0.08 ng/mL; follicle-stimulating hormone level, 24.92 mIU/mL; estradiol level, 36.21 pg/mL; prolactin level, 34.57 ng/mL. Exploratory laparotomy was performed; an approximately 11-cm-sized cystic mass with a smooth surface and focal solid component containing pus-like fluid was seen in the right ovary. The uterus and left ovary were not properly visible owing to the presence of severe adhesions between the rectum, bladder, and omentum. Right salpingo-oophorectomy and partial omentectomy were performed, followed by retrograde pyelography and ureteroscopy-guided double-joint stent insertion. Microscopic examination of the ovarian tumor showed characteristic histologic features of dysgerminoma, i.e., large round or polygonal tumor cells and lymphocytes in the intervening stroma (Fig. 2). A chromosome study revealed a normal female karyotype (46, XX). After surgery, positron emission tomography-computed tomography revealed an enlarged lymph node with mild fludeoxyglucose uptake in the precaval area (L3 level) and slightly enlarged lymph nodes in the left para-aortic area. Radiologic findings indicated metastatic lymphadenopathy. Therefore, 6 cycles of chemotherapy with bleomycin (15 mg/body surface area [BSA]), etoposide (100 mg/BSA), and cisplatin (20 mg/BSA) were completed, and the patient responded well to the treatment. During the 6-year follow-up, there was no evidence of recurrence.
Fig. 1
Abdomino-pelvic computed tomography. (A) Axial view showing a large (10 cm) right ovarian tumor (arrow) with internal necrosis, possibly complicated by colo-ovarian fistula and associated pelvic inflammatory disease. (B) and (C) coronal view showing uterus didelphys (arrowhead) and left lower ureteral stricture with minimal left hydronephroureterosis. Non-visualization of the right kidney indicates right renal agenesis (asterisk).
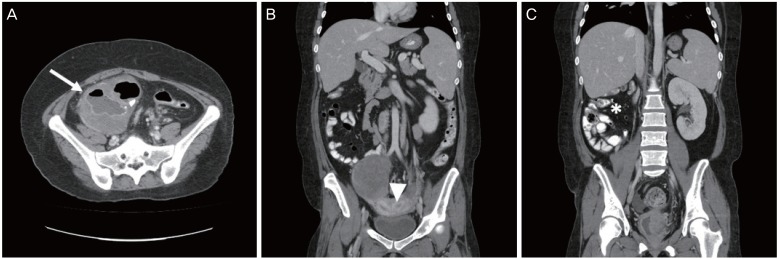
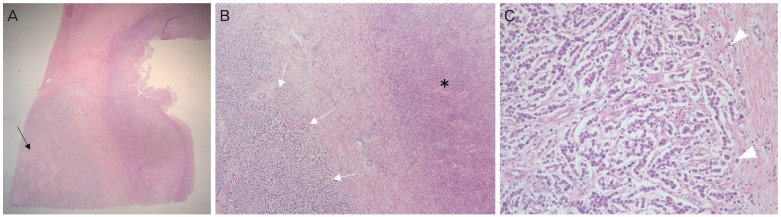
Fig. 2
Pathologic findings. (A) Microscopic findings of the right ovarian mass. In the left lower corner, a dysgerminoma tissue is identified along with an abscess cavity along the right side (black arrow) (Hematoxylin and eosin stain, ×12.5). (B) The areas of dysgerminoma (white arrows) and abscess (asterisk) are adjacent to each other (×40). (C) Characteristic histologic features of dysgerminoma, such as large round or polygonal tumor cells and lymphocytes in the intervening stroma (white arrowheads), are noted (×200).
Discussion
Müllerian anomalies are often recognized after the onset of puberty when a young girl has menstrual disorders or when a reproductive-aged woman encounters infertility and obstetric complications, such as abortion or preterm labor. Uterine anomalies are the most common congenital malformation of the female genital tract [3]. The most common Müllerian anomalies include uterus didelphys, bicornuate uterus, and septate uterus [3]. In the present case, the patient with secondary amenorrhea was diagnosed with uterus didelphys. Urinary tract anomalies are the most common abnormality in Müllerian anomalies, and the incidence of renal anomalies associated with genital abnormalities is 25% to 89% [4]. Unilateral renal agenesis is the most common abnormality and is most frequently associated with uterus didelphys [5]. In this case, the patient had uterus didelphys with right renal agenesis. Müllerian anomalies accompanied with urinary tract abnormalities are common; however, gynecologic malignancies with Müllerian anomalies are rare.
Dysgerminoma accounts for less than 1% of all ovarian neoplasms and usually occurs in adolescents or young women in the 2nd to 3rd decades of their lives [6]. Most patients with dysgerminoma often present with abdominal pain, abdominal distension, or pelvic or abdominal mass [6]. Approximately 5% of dysgerminomas are found in women with chromosomal abnormalities, such as 46XY (testicular feminization or Swyer syndrome) or 45X/46XY mosaicism [7]. However, dysgerminoma with uterine anomalies has not been reported. In this case, the patient with a normal female karyotype presented to our hospital with secondary amenorrhea with abdominal pain and was diagnosed with dysgerminoma with uterus didelphys.
Gynecologic malignancies with Müllerian anomalies are very rare. Gao et al. [3] reported 3 cases of endometrial cancer with congenital uterine anomalies. They mentioned the possibility that endometrial cancer is not detected by endometrial biopsy with coexisting uterine malignancies and uterine anomalies in patients with abnormal vaginal bleeding. They recommended the use of magnetic resonance imaging. Dysgerminomas with Müllerian anomalies are also very rare; however, the tumors can be diagnosed well by ultrasonography or APCT. The treatment of dysgerminoma differs depending on the stage. In the present case, the patient underwent 6 cycles of adjuvant chemotherapy with bleomycin, etoposide, and cisplatin. Platinum-based chemotherapy has complications including renal toxicity or fertility impairment. When we consider the treatment of dysgerminoma in patients with Müllerian anomalies with renal agenesis, attention should be paid to renal toxicity.
In conclusion, to the best of our knowledge, this is the first reported case of dysgerminoma with uterus didelphys. The diagnosis of ovarian dysgerminoma with uterus didelphys is not difficult; however, more careful treatment is needed in patients with advanced-stage dysgerminoma with Müllerian anomaly than in patients without Müllerian anomaly.
 XML Download
XML Download