

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
“Recommit to do everything in our power to reduce the cesarean rate” was the statement given by Richard N. Waldmam in the inaugural address of the Annual Clinical meeting of the American College of Obstetrics & Gynecology (ACOG) in 2010 [1]. For most of the 20th century, the cesarean rate hovered between 1–5% [2] and was performed only in life-threatening situations, as the procedure is risky and the prevalence of the dictum that “once a cesarean always a cesarean.” With the improvement in surgical techniques, advancement in anesthesia and antibiotics, cesarean sections have become a safer option. Thus, the cesarean rate rose from 5% in 1970 to 31.1% in the USA and 25.5% in the UK by 2012 [3]. According to the international healthcare community, the cesarean section rate should be curtailed to 10–15% cases, where it has a definite role in decreasing maternofetal morbidity and mortality, rather than beguiling it without indication [45]. After the appraisal of the cesarean epidemic and complications, the Royal College of Obstetricians and Gynecologists (RCOG)/National Institute for Health and Care Excellence, ACOG/National Institutes of Health determined that planned vaginal birth after cesarean section (VBAC) is a safe option for most women with one previous lower segment cesarean delivery, which is also affirmed by the health economic model [3]. Despite VBAC acceptance, “how to give trial in cases with an unfavorable cervix” was the matter of concern for obstetricians. Although the role of oxytocin, artificial rupture of membranes, Foley's catheter, and prostaglandins were duly studied, the guidelines regarding the mode of labor induction in patients with previous cesarean are still equivocal. Cochrane 2017 reviews the methods of term labor induction for women with a previous cesarean section is still inconclusive for a lack of adequate research.
We did this work to study obstetric outcomes in post cesarean patients undergoing induction of labor with prostaglandin E2 (PGE2) gel compared with patients who developed spontaneous labor pains. The null hypothesis was that there is no difference in the outcome. The outcome measures included successful VBAC, failed VBAC, scar dehiscence, scar rupture, and the maternofetal outcome.
Materials and methods
This is a retrospective case control study that was conducted under the Department of Obstetrics and Gynecology in a tertiary care rural teaching hospital over the span of one year. Patients who underwent one previous lower segment cesarean section (LSCS) with a period of gestation of 34 weeks or more eligible for trial of labor after cesarean section (TOLAC) were included in the study group. Medical records of these patients were analyzed for details like obstetric history, mode of onset of labor, induction process, labor process, mode of delivery, and maternofetal outcome. These patients were further divided into 2 groups: patients who experienced spontaneous labor pain were included in group 1 and patients who underwent induction of labor with PGE2 gel (0.5 mg inopportune BP per 3.0-gram gel) were included in group 2. A maximum of 3 doses of gel administered in 6-hour intervals were used to induce labor. Oxytocin was used for augmentation in both groups when indicated under strict monitoring.
The fetus was monitored via continuous electronic fetal monitoring and patients were monitored for impending rupture by evaluating pulse rate and suprapubic palpation for scar tenderness in the post contraction phase. Patients developing tachycardia, fetal distress, or tenderness in the suprapubic area immediately underwent surgery with a provisional diagnosis of an impending scar rupture. The primary outcome of the study was rate of successful VBAC, difference in incidence of rupture uterus, and neonatal outcome for both groups.
The standard definitions of successful VBAC were defined as successful vaginal delivery with or without instrumentation. Failed VBAC was defined as when a patient delivered abdominally irrespective of indication and stage of LSCS. The term scar dehiscence was used when a clear rent was noted at the site of the previous scar involving muscular layers of the uterine wall intraoperatively. Uterus rupture was diagnosed when signs of alteration in the vitals of the patient, fetal distress, bleeding per vagina, or superficial palpation of fetal parts were evident.
Descriptive statistics were used to calculate the mean and standard deviations. To calculate P-values, an independent sample t-test was used for continuous variables while the χ2 test was used for categorical data. Fisher's exact test was used when the expected frequency was less than 5. A P-value of less than 0.05 was considered statistically significant. Univariate analysis performed using SPSS 20 (IBM Corp., Armonk, NY, USA).
Results
In total, 5,203 patients delivered during the study period, among which 498 had a history of one cesarean section. A total of 335 patients were selected for TOLAC and the remaining patients underwent an elective repeat cesarean section (ERCS). They were further divided into 2 groups, depending on the mode of onset of labor pains, i.e., spontaneous and induced. Table 1 encompasses the characteristics of both groups.
Table 1
Characteristics of patients in both the groups
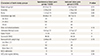
The mean duration of previous cesarean sections was 38.42±2.25 months in group 1 and 38.38±2.43 months in group 2; this difference was not statistically significant (P=0.97). The rate of operative vaginal delivery was 0.018% and 0.017%, respectively, for each group. In group 1: 81 (37%) patients experienced obstetric complications, including preterm labor pains (29), premature rupture of membranes (PROM; 21) preeclampsia (16), and intrauterine growth restriction (IUGR; 15). In group 2, 49 (42.65%) patients experienced obstetric complications such as preeclampsia (15), PROM (7), preterm PROM (16), and IUGR (11). Both groups were comparable statistically (P=0.182). The most common indication for induction of labor in descending order was term gestation (39–42 weeks, 58%), preterm PROM and PROM (17.5%), preeclampsia, and IUGR and oligohydramnios (25.21%). The mean period of gestation for induction was 38.73±1.4 weeks. The indications of previous LSCS for both the groups included malpresentations (32.8%), fetal distress (19.7%), lack of labor progression (17.46%), failed induction (7.46%), and others, including antepartum hemorrhage, IUGR, and unknown causes (22.4%). Previous LSCS was performed as an emergency procedure in 80% of the cases. Both groups were comparable for type and indications of previous LSCS. There was a history of contraception use in 27 patients in group 1 and 14 patients in group 2. Spontaneous abortion was also reported in 25 patients in group 1 and 22 patients in group 2.
Table 2 compares the indications of repeat cesarean sections in both groups with intraoperative findings. In patients with spontaneous labor pains, fetal distress was an indication of repeat LSCS in 45% of patients (3 were preterm, 3 developed severe preeclampsia, 1 IUGR, and 1 patient had scar dehiscence intraoperatively) and in 31% of patients, an impending scar rupture was the indication (7 patients had normal scars but dense adhesions were present and 2 patients had scar dehiscence of 2–3 cm). However, in group 2, 44% of the patients had failed induction (5 patients had failed induction in a previous pregnancy, 4 patients had a previous cesarean for malpresentation, and 2 for eclampsia) and 27% patients underwent surgery for fetal distress, out of which 2 patients had scar dehiscence. Among eight patients that presented impending scar rupture, 3 patients experienced scar dehiscence. In the cases of scar rupture, a hemoperitoneum of 750–1,000 mL with vaginal bleeding and a fresh still birth was noted, demanding the repair of rent.
Table 2
Indications for repeat lower segment cesarean section (LSCS) and intraoperative findings

The intergroup variants among the patients who delivered vaginally and by LSCS were compiled as reflected in Table 3.
Table 3
Univariate analysis of group 1 & 2

A statistically significant difference in the Bishop score was noted in the patients with successful VBAC compared to patients who underwent repeat cesarean section. The dose of gel used in group 2 was 1.65±0.75 in the successful VBAC group and was 2.04±0.77 in patients who underwent repeat LSCS; the P-value was 0.005.
Discussion
Of the 335 cases that were selected for TOLAC, 265 had successful VBAC constituting a total VBAC rate of 79.10% at our institution. Metanalysis by Guise et al. [6] and Mozurkewich and Hutton [7] (n=103,188 VBAC labors) also reported a pooled VBAC labor success rate of 74%, while the National Institute of Child Health and Human Development study reported a 73% VBAC rate (n=17,898 VBAC labors) [3]; these are comparable to the present study. A post-cesarean vaginal birth rate of 64% [8] to 68.3% [9] has been reported in patients after induced labor with prostaglandin gel. In our study, the reported rate was 64.34%. The rate of successful VBAC in patients with spontaneous onset of labour pains is reported from 67.2% [9] to 72.3% [10]; in present study it was 86.82%.
Literature has suggested that maternal age, birthweight, and parity are some of the key factors in determining success of TOLAC. Doshi et al. [11] and others [1213] reported the interesting finding that maternal age >35 years and fetal weight >3.5 kg were associated with decreased chances of successful TOLAC. In the present study, the mean age was 25.81±2.72 years, which is younger that reported in literature from the western world [8] but comparable with that reported in studies of Asian countries [910]. This may be due to nutritional, financial, or ethnical factors that vary among these regions. According to the RCOG guidelines, a previous VBAC is the single best predictor for successful TOLAC and is associated with a planned VBAC success rate of 85–90% [3] and is also independently associated with a reduced risk of uterine rupture [3]; however, in the present study, the average parity was 1.371±0.713, reflecting a dominance of primiparous patients. The odds ratio (OR) for successful TOLAC with a prior vaginal delivery is 3.90 (95% confidence interval [CI], 4.35–5.26) while it is 4.76 (95% CI, 4.35–5.26) with prior successful TOLAC [14]. In the present study, the number of patients with prior vaginal delivery was comparable between the groups.
The factors where variations in both groups were statistically significant include bishop score at admission, mode of delivery, and neonatal outcome. Abdelazim et al. [15] reported that cervical dilatation of 4 cm or more favors successful TOLAC and shortens the duration of labour. Harper et al. [16] reported that unfavorable initial cervical examination increases the risk of uterine rupture. Women with spontaneous labor cervical dilation of 4 cm or more are more likely to have successful TOLAC than women without these characteristics (OR for successful TOLAC with spontaneous labor, induction, augmentation 1.0, 0.50, and 0.68, respectively; for admission cervical examination >4 cm, 2.56, 95% CI, 2.38–2.67) [1317]. The difference in bishop score at admission was statistically significant in patients with successful TOLAC compared to failed TOLAC in both the groups, as shown in Table 3. Therefore, a favorable cervix is the key factor in deciding the success of TOLAC.
PGE2 has been reported as a time-tested tool of cervical ripening and labor induction for an unfavorable cervix (level 1 evidence) by Society of Obstetricians and Gynecologists of Canada [18]. A systematic review on labor induction in patients without cesarean section and found that PGE2 gel and vaginal misoprostol were more effective than oxytocin in causing vaginal delivery within 24 hours but are also associated with an increased incidence of uterine hyperstimulation. Mechanical methods like using an intracervical Foley's catheter reduces uterine hyperstimulation and are acceptable methods of induction in patients with one previous LSCS (level 1B) but are associated with increased maternal and neonatal infections, and hence, morbidity [1819]. Data supporting the use of PGE2 is inconsistent and recommendations are contradictory. The use of PGE2 gel for cervical ripening was reported as safe with no increased risk of uterine rupture [892021]. The ACOG recommends PGE2 only for women with good chances of successful VBAC, quoting studies presenting both pictures [2223]. The French guidelines recommend cautious use of PGE2 after due consideration of the chances of success and taking all relevant obstetric and maternal factors into account [2223].
RCOG reported (level B evidence) that planned VBAC is associated with a 1 in 200 (0.5%) risk of uterine rupture. RCOG guidelines 45 reported a 2- to 3-fold increased risk of uterine rupture and around 1.5-fold increased risk of cesarean delivery in induced or augmented labor compared to spontaneous labor pains in patients of TOLAC. In the present study, the results are comparable to RCOG literature.
In contrast to uterine rupture, uterine scar dehiscence is a more common event and seldom results in maternal and fetal complications. Uterine dehiscence is considered a benign condition compared to uterine rupture. A review article by Bharatam [24] mentioned the incidence of cesarean scar defect between 6.6–69% with variations due to the absence of criteria for cesarean scar dehiscence. In a meta-analysis in 2015, the reported incidence was 1.9% [24]. In the present study, it was 4% in the induced group and 1% in the spontaneous group. The high rate of impending scar dehiscence does not rule out the use of gel but necessitates the availability of good maternofetal monitoring at a continuous cesarean facility.
Although, in the present study, the difference of neonatal outcomes between the 2 groups were statistically significant. However, the main reason for nursery admission was prematurity in both groups. According to RCOG guidelines, planned preterm VBAC had similar success rates to planned term VBAC but with a lower risk of rupture [3]. In the present study, no dehiscence and rupture were noted in preterm patients. In all the reviewed guidelines, more cases of perinatal mortality and neonatal mortality are found for VBAC than for ERCS. The reason may be neonatal sepsis, especially in patients who undergo LSCS after TOLAC failure and uterine ruptures [23]. In the present study, the neonatal mortality was 0.5% and the neonatal morbidity was mainly for prematurity and IUGR.
The famous saying, “nothing can be purely black and white, everything has grey shades” holds true in the process of labor induction for TOLAC. It is well documented that the incidence of induction of labor in the U.S.A. increased steadily, where elective inductions accounted for a greater proportion of these cases [25]. Same practice is for TOLAC with unfavorable cervix as majority of patients were induced for postdatism and PROM where one cannot wait further and need to intervene. At present, there are no clear-cut guidelines for the use of PGE2 gel and its dose. Retrospective studies suggest that low-dose PGE2 is a safe option for labor induction in women undergoing TOLAC. The Cochrane review published in 2017 found it insufficient and encouraged further research.
In conclusion, the present study reflects that a supervised induction with prostaglandins is a safe and effective option without a significant difference in morbidity and mortality. However, a small sample size and other limitations mentioned below require a further larger study or randomized control trial to answer the final question.
The limitations of study include its retrospective nature and the inclusion criteria, like prematurity and severe preeclampsia. At times, it is difficult to assess whether admission in NICU is because of prematurity or due to complications of TOLAC. Moreover, sometimes the induction process was terminated prematurely if preeclampsia progressed from mild to severe. These factors bear potential soil to germinate bias and errors. Lack of availability of previous records is also another limitation because of the patients-related factors that may not have been considered.
 XML Download
XML Download