

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
There are 2 types of dysmenorrhea: primary and secondary. Primary dysmenorrhea typically occurs with no associated pelvic pathology, and is common in adolescents and young women [1]. The prevalence of primary dysmenorrhea ranges from 60–93% [2]. Secondary dysmenorrhea is due to an organic pathology in the uterus, such as endometriosis. The risk factors for primary dysmenorrhea are an age younger than 20 years, a family history of dysmenorrhea, smoking, heavy bleeding, irregular bleeding, menarche age younger than 12 years, low body weight, and nulliparity [234]. The cause of pain in primary dysmenorrhea is excess production of prostaglandins in the uterus during the ovulatory cycle, which leads to uterine contraction and ischemia [5]. Nonsteroidal anti-inflammatory drugs (NSAIDs) and oral hormonal contraceptives are suggested for reducing the symptoms of dysmenorrhea; however, these drugs can have serious adverse effects in some women [6]. NSAID therapy can increase renal, cardiovascular, and gastrointestinal complications. The most common gastrointestinal complications include heartburn, stomach pain, nausea, vomiting, diarrhea, and constipation [7]. Various studies have reported on alternative and complementary medicine methods for relief of primary dysmenorrhea, including herbal and dietary therapies, behavioral interventions, acupressure, spinal manipulation, transcutaneous electrical nerve stimulation, and acupuncture [589].
Amiri Farahani et al. [10] have shown that honey and mefenamic acid capsules had a similar pain relief effect among women with primary dysmenorrhea; a study by Golder [11] found that bee propolis improved chronic backache and hip pain as well as fresh injuries to muscles and tendons.
Bee propolis has been used in traditional Iranian medicine for relieving menstrual pain [12]. Recent studies have reported that propolis contains elevated amounts of a certain type of isoflavonoid, i.e., isoflavones. This particular group of polyphenols exhibits a wide range of biological properties, including antiviral, antimicrobial, anti-inflammatory, and even anticancer activities [1314]. Three derivatives of p-coumaric acid isolated from a Brazilian sample have shown a relaxant effect on smooth muscle by propolis [15]. Therefore, propolis can be effective in reducing uterine pain through its anti-inflammatory and antispasmodic effects [1617].
As for the trend of women to use herbal drugs and not preform of similar study in the Iran, therefore, the present study was conducted to evaluate the effect of bee propolis compared with placebo on primary dysmenorrhea in students from Hamadan University of Medical Sciences.
Materials and methods
1. Study design
The present study was a double-blind randomized controlled trial conducted on 86 students from the Hamadan University of Medical Sciences (Hamadan, Iran) in 2018.
The students were randomized to 2 treatment groups by a computer program using the rand command. The placebo group received a 500-mg starch capsule taken daily from 2 days before menstruation until the third day of menstruation, for 2 cycles. The bee propolis group received a 500-mg bee propolis capsule (Shahd Golha Honey Company, Isfahan, Iran) taken daily from 2 days before menstruation until the third day of menstruation, for 2 cycles.
2. Eligibility criteria
We included students with the following criteria: 1) single; 2) 19–23 years of age; 3) a history of regular menstruation; 4) use of no other medication for alleviation of dysmenorrhea; 5) no use of hormonal drugs; 6) no clinical history of major psychological disorders; 7) consecutive menstrual cycles; and 8) pain score 3 and higher based on visual analog scale (VAS). Exclusion criteria were intolerance to drug use and improper use of drugs or use discontinuation. Ultrasound was used to rule out secondary dysmenorrhea. All students provided written consent.
3. Participant characteristics
We used a researcher-designed questionnaire including age, menarche age, and body mass index (BMI). The students completed a baseline assessment using a 10-mm VAS for evaluating pain, with 0 representing no pain and 10 representing the worst possible pain.
4. Sample size
According to the sample size in similar interventional studies on primary dysmenorrhea [18] and with the probability of anticipating a 10% loss to follow-up, b=0.2 and a=0.05, the number of participants required was estimated to be 86 in total, with 43 students in each group according to the inclusion criteria.
5. Data analysis
The quantitative variables are presented as mean±standard deviation. Normality of data was assessed using the Kolmogorov–Smirnov test. Continuous variables between the two groups were compared using Student's t-test. All the analyses were conducted using SPSS (version 23) (IBM Corp., Armonk, NY, USA). We considered a P-value of less than 0.05 as significant.
Results
In this study, of 126 students evaluated for eligibility, 40 did not meet the inclusion criteria, and thus were excluded. Therefore, a total of 86 students (43 per group) were included, of which 3 in the placebo group did not return for follow-up. Thus, 43 students in the bee propolis group and 40 students in the placebo group were evaluated (Fig. 1). The mean ages of the students in the placebo and bee propolis groups were 21.32±1.30 and 21.07±1.58 years, respectively; the mean menarche ages in the placebo and bee propolis groups were 12.15±1.23 and 12.48±1.30 years, respectively; and the mean BMIs in the placebo and bee propolis groups were 24.27±2.40 and 23.51±3.03 kg/m2, respectively. There was no significant difference between the 2 groups in baseline characteristics (Table 1).

Table 1
Characteristics of students in both groups
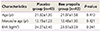
| Characteristics | Placebo group (n=40) | Bee propolis group (n=43) | P-value |
|---|---|---|---|
| Age (yr) | 21.32±1.30 | 21.07±1.58 | 0.410 |
| Menarche age (yr) | 12.15±1.23 | 12.48±1.30 | 0.421 |
| BMI (kg/m2) | 24.27±2.40 | 23.51±3.03 | 0.241 |
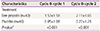
Table 2 presents pain scores before and at the first and second months after the intervention in the placebo and bee propolis groups. The means of the pain scores in the bee propolis group were 5.32±2.28 and 4.74±2.40 in first and second months after the intervention, respectively, whereas the means of the pain scores in the placebo group were 7.40±1.21 and 7.17±1.24 in first and second months after the intervention, respectively. A significant change was found in the mean pain scores during the first (P<0.001) and second (P<0.001) months after using bee propolis compared with placebo. Table 3 shows the comparison of changes in dysmenorrhea scores between the first (cycle 0–cycle 1) and the second (cycle 0–cycle 2) cycles, which were significant (P<0.001). In present study, no adverse effects were reported after bee propolis use.
Table 2
Comparison of changes in mean dysmenorrhea scores in both groups

Discussion
Our study showed that the daily use of a 500-mg capsule of bee propolis compared with placebo decreased primary dysmenorrhea during the first and second months after use. Therefore, it can be an alternative to NSAIDs for relief of primary dysmenorrhea; no adverse effects were observed during its use.
Until now, no studies about the effect of bee propolis on dysmenorrhea had been conducted; however, some studies had shown the effect of honey on relief of primary dysmenorrhea. A study by Amiri Farahani et al. [10] in Iran was conducted for comparison of honey with mefenamic acid for pain relief among women with primary dysmenorrhea. They reported that honey and mefenamic acid capsules had a similar effect for pain relief [10]. In 2004, Meda et al. [3] reported that honey and honeybee larvae were used for treating period pains and postnatal disorders among women; Golder [11], also in 2004, reported that bee propolis treated chronic backache, hip pain, and fresh injuries of muscles and tendons.
Another study reported on traditional methods for relief of dysmenorrhea. This study evaluated the effect of Menstrugole on primary dysmenorrhea. They reported a significant change in the mean pain score during the first and second cycles after the use of Menstrugole compared with the placebo. Therefore, Menstrugole decreased pain severity in female students [8].
This study had some limitations. For example, the small sample size; the difference between the trial groups with less possibility of random error was observed by the sample size of large. Another limitation was the short study period. We evaluated adverse effects of bee propolis use for only 2 months. Therefore, there could be a possibility of bias. Also, this study was performed on single adolescents and cannot be generalized to other age groups. Therefore, we suggest that further studies be conducted in other countries and in different age groups.
Traditional methods have been preferred by Iranian women to modern methods for relieving primary dysmenorrhea, and the present study showed that bee propolis is effective for relief of this pain. Most NSAIDs used in long-term therapy have exerted severe adverse effects [19]; however, bee propolis showed no adverse effects. Therefore, bee propolis can be used as an alternative to NSAIDs for relief of primary dysmenorrhea.
In conclusion, our study showed that the use of bee propolis for 2 months compared with placebo reduced primary dysmenorrhea during the first and second months after use, with no adverse effects. Therefore, it can be used as an alternative to NSAIDs for relief of primary dysmenorrhea.
 XML Download
XML Download