

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
From the outset of surgical interventions, development of minimally invasive treatment modalities has been an area of consistent focus, with efforts to minimize postoperative pain. However, rather than postoperative pain, studies showed that the most uncomfortable experiences associated with general anesthesia are nausea and vomiting immediately after surgery. This indicates that postoperative nausea and vomiting (PONV) have a significant effect on patients [1].
PONV may induce electrolyte imbalance, and excessive stress of muscles involved in the gag reflex, which can damage the esophagus or larynx, and result in pneumothorax or aspiration pneumonia [2]. Theses complications ultimately delay postoperative recovery and cause great discomfort.
In 1995, Rowbotham [3] reported that PONV occur at an incidence of 36%. The most prevalent patient group that reported PONV consisted of those who underwent obstetric and gynecological surgeries (42%).
The incidence of PONV is relatively higher in patients who have undergone laparoscopy-assisted gynecological surgeries [4]. However, compared with laparotomy, the laparoscopic approach shortens the length of hospital stay and recovery period, lowers the incidence of intra-abdominal adhesion, and reduces blood loss volume. Therefore, it remains a mainstream modality in the treatment of benign gynecological diseases [56]. Single-port laparoscopy-assisted surgery, which is frequently performed in Korea, causes less postoperative pain and produces excellent aesthetic outcomes and is thus preferred by most patients [78]. Therefore, efforts to prevent PONV in patients undergoing single-port laparoscopy-assisted gynecological surgeries are reasonable.
Anticholinergics, antihistamines, butyrophenones, and dopamine receptor antagonists are often effective in preventing and treating PONV. However, such drugs can produce adverse effects such as excessive analgesia, hypotension, xerostomia, and extrapyramidal tract syndrome [9]. In recent years, 5-hydroxytryptamine type 3 (5-HT3) receptor antagonists have been studied.
Ramosetron (Nasea, Astellas Pharma, Tokyo, Japan) is a recently developed selective 5-HT3 receptor antagonist that has a higher receptor binding affinity than ondansetron, granisetron, and dolasetron, which are conventional forms of 5-HT3 receptor antagonists. Moreover, it has a longer duration of action and is effective in treating nausea and vomiting related to anticancer therapy, and in preventing PONV [10]. The most effective postoperative dose and route of administration of ramosetron [11], and its optimal timing of administration have been investigated [12]. However, no current recommended protocol exists to control PONV in high-risk patients.
Numerous anesthesiologic studies with short-term follow-up have been performed to examine nausea and vomiting after a single-dose administration of ramosetron directly after surgery in the recovery room. However, owing to the short-term observation of the effectiveness of ramosetron, the evaluation of the effects of a regular administration of ramosetron in hospitalized obstetrics and gynecology patients has limitations. No studies have evaluated the ongoing effects of ramosetron injections for preventing and treating PONV after a single-port laparoscopy-assisted gynecological surgery.
Therefore, we conducted this prospective randomized controlled study to examine the effects of intravenous injections of ramosetron for preventing PONV in patients undergoing single-port access total laparoscopic hysterectomy (SPA-TLH).
Materials and methods
The present study was conducted in compliance with the ethical guidelines of our medical institution, which included registration at clinicaltrials.gov (NCT 02011659). Patients who underwent elective SPA-TLH under general anesthesia at the National Health Insurance Service Ilsan Hospital between June 2013 and July 2014 were enrolled in the present study.
The inclusion criteria were as follows: age between 18 and 70 years, and American Society of Anesthesiologists physical status class I or II. The exclusion criteria were as follows: history of drug abuse; drug hypersensitivity; gastrointestinal, cardiovascular, respiratory, cerebral, renal, or hepatic diseases; severe motion sickness; pregnancy; lactation; previously use antiemetics within 24 hours; current smokers; and those deemed unfit for study participation according to the investigators' judgment.
A difference of 0.8 in the Nausea Vomiting Scale was considered clinically relevant. Type 1 and 2 errors were set to the usual levels of 0.05 and 0.2., respectively. Assuming a 10% withdrawal rate, the number of cases needed per group was approximately 45. Randomization was based on computer-generated random sampling numbers.
Ninety patients were enrolled in the present study. The patients were randomized via generation of random number tables to receive ramosertron or normal saline (placebo) as they were transferred to the ward. They received treatment or placebo during the first 24-hour postoperative recovery period.
1. Study protocol
All the patients received one prophylactic intravenous injection of cephalosporin 1 g, a second-generation antibiotic, 30 minutes preoperatively. The patients received pre-anesthetic intramuscular injection of glycopyrrolate 0.2 mg and midazolam 0.05 mg/kg 1 hour preoperatively. The patients received a 1-minute infusion of remifentanil 1 μg/kg for induction of anesthesia with 100% oxygen via a face mask. After confirmation of loss of consciousness, propofol 2 mg/kg was intravenously (IV) administered along with an intravenous injection of rocuronium 0.6 mg/kg. Thereafter, anesthesia was maintained using sevoflurane. Single-port laparoscopy-assisted total hysterectomy was performed as previously described [13]. Prior to the completion of surgery, the patients were administered ramosetron 0.3 mg IV followed by ketolac 0.5 mg/kg and antagonists (pyridostigmine 10 mg and glycopyrrolate 0.2 mg). After the confirmation of recovery of consciousness, the patients were transferred to the recovery room. Fentanyl 20 μg/kg was diluted in 100 mL of saline for 48-hour infusion of patient-controlled analgesia (PCA). Fentanyl was administered at a basal rate of 2 mL/hour with a l-mL bolus and 15-minutes lockout time. After the patients were transferred to the ward, they were randomly assigned to 2 groups and administered ramosetron 0.3 mg or placebo IV at 12- and 24-hour postoperative time points. The study personnel who performed the study treatments were blinded to the patients' identities. Thus, the study was conducted in a double-blinded manner (Fig. 1).

2. Outcome measures
The operation time, blood loss volume, and intraoperative damage to vital organs such as the bowel and bladder were recorded. The patients were evaluated for severity of PONV at 6, 12, 24, and 48 hours postoperatively. PONV was defined as nausea, retching, and/or vomiting symptoms. Each symptom was subcategorized for evaluation. Nausea was defined as an unpleasant feeling of vomiting. Retching was defined as an excessive contraction or a regular movement of the respiratory muscles where no gastric contents were excreted, and vomiting was defined as the excretion of gastric contents. Nausea and vomiting were quantified using the numerical rating scale (NRS; 11-point rating, 0–10), which enabled the patients' subjective symptoms to be evaluated. Observers were blinded to the identity of the patients. Intravenous injection of metoclopramide 10 mg was administered as a rescue antiemetic to vomiting patients and those with an NRS score of ≥4 points who wanted to control their PONV symptom. The patients were evaluated 2 hours after metoclopramide administration. If the symptom persisted, PCA administration was discontinued in each patient. Use of additional antiemetics and discontinued treatment with PCA were documented.
Patients with postoperative pain management NRS score of ≥5 points were advised to press the PCA bolus button. Two hours after administration of PCA bolus, the patients were reevaluated, and those with persistent symptoms were given ketolac 30 mg via intravenous injection. If no effect was observed 2 hours after the ketolac injection, the patients were given an intravenous injection of pethidine 25 mg.
Hemoglobin and hematocrit levels were checked 1 and 3 days postoperatively. The hospitalization duration from surgery to discharge and any complications such as headache, dizziness, constipations, or other serious complication were also evaluated.
3. Statistical analysis
Statistical analysis was completed using SPSS version 13.0 (SPSS Inc., Chicago, IL, USA). Age, body mass index (BMI), operation time, period of anesthesia, and NRS scores were analyzed using an independent t-test. The incidence of PONV, use of rescue antiemetics, discontinued use of PCA, and postoperative complications were analyzed using the Pearson χ2 and Fisher exact tests. All measurements were expressed as mean±standard deviation or percentage (No. of patients). A P-value of <0.05 was considered statistically significant.
Results
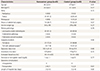
No significant differences in age, BMI, medical history, or surgical indications and modalities were found between the 2 groups. No significant differences in intraoperative time, anesthetic time, or estimated blood loss were found between the 2 groups (Table 1).
Table 1
Clinical characteristics and postoperative data
Patients who experienced symptoms of nausea, retching, or vomiting during the 48-hour postoperative period were considered cases of PONV. The overall incidence of PONV showed no statistical significance at 46.7% in the experimental group and 51.1% in the control group (Table 2). The incidence of PONV was highest at the 12-hour postoperative time point in both groups but showed no statistical significance (Fig. 2). At 24 and 48 hours post surgery, the incidence of PONV based on NRS score was significantly lower in the experimental group than in the control group (P=0.04; experimental group vs. P=0.03; control group). By contrast, no significant difference in the severity of postoperative pain was observed between the 2 groups (Table 3). No significant difference was also found in the incidence of adverse effects after administration of ramosetron in each group (Table 4).
Table 2
Incidence of postoperative nausea and vomiting (PONV)


Table 3
Numeric rating scale of postoperative nausea and vomiting (PONV) and postoperative pain
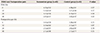
Table 4
Side effects of ramosetron injection

| Symptoms | Ramosetron group (n=45) | Control group (n=45) | P-value |
|---|---|---|---|
| Headache | 7 (15.5) | 9 (20.0) | 0.63 |
| Dizziness | 6 (13.3) | 7 (15.5) | 0.77 |
| Constipation | 8 (17.8) | 7 (15.5) | 0.72 |
The frequency of the use of postoperative rescue antiemetics was 26.7% in the experimental group and 48.9% in the control group, which indicates that PONV was significantly lower in the treatment group (P=0.02). Notably, PCA discontinuation and the additional use of analgesics showed no significant difference between the 2 groups (Table 5).

Discussion
The field of gynecology has evolved with a remarkable advancement in technology and studies in single-port laparoscopy-assisted surgery [814]. The advantages of laparoscopy-assisted surgery, including less postoperative pain, great aesthetic effects, and rapid postoperative recovery, are generally acknowledged. However, PONV still remains an issue that must be addressed during the postoperative recovery period. Despite prophylactic measures, the incidence of PONV during the 24-hour postoperative period is approximately 30% and can reach 70% in high-risk patients [15].
The etiological factors for the pathogenesis of PONV include individual factors (female sex, age [<50 years], non-smoking, obesity, and history of nausea, vomiting, or motion sickness), surgical factors (otolaryngological surgery, breast surgery, strabismus surgery, laparoscopy-assisted surgery, and gynecological surgery) [416], and anesthetic factors (inhalation anesthetics, N2O, opioid analgesics, and high-dose neostigmine) [17]. Postoperative pain and preoperative and postoperative dehydration may also increase the incidence of PONV [18].
In our study, the overall incidence of PONV was 46.7% in the experimental group and 51.1% in the control group, which were relatively higher than the results reported in other studies. Most patients who experience PONV have at least 2 predisposing factors [17]. In this study, all the patients were non-smoking women who underwent laparoscopic gynecological surgery and received PCA, which place them in the moderate- to high-risk category.
Vomiting occurs from 5 different receptors, namely dopamine, acetylcholine, histamine, serotonin receptors, and neurokinin 1-substance P. However, PONV is usually caused by 1) stimulation of the vomiting center through visceral fiber irritation and postoperative retention in the intestine, and 2) opioid and inhalation anesthesia directly stimulating the chemoreceptor trigger zone, which then stimulates the vomiting center through the release of dopamine and serotonin [1517]. The 5-HT3 antagonist agents affect these 2 pathways to effectively prevent PONV.
Previous studies demonstrated that ramosetron 0.3 mg prevents PONV more effectively than ondansetron 8 mg [1920]. Kim et al. [21] conducted a meta-analysis of randomized controlled trials, focusing on the efficacy of palonosetron (0.075 mg), a newly developed second-generation 5-HT3 antagonist, and ramosetron (0.3 mg) for preventing PONV. However, the results showed no definite differences in effectiveness and safety between the 2 agents.
Review of the literature revealed that the best route of administration for ramosetron is intravenous or intramuscular gradual injection of a single dose. According to Tang et al. [22] and Sun et al. [23], administration of 5-HT3 immediately prior to the completion of surgical procedure is more effective. In addition, Cruz et al. [24] reported that administration of the drug 30 minutes before the completion of the surgical procedure is more effective. This shows several differing recommendations regarding the most effective delivery time of 5-HT3 administration.
To minimize the bias associated with the surgical methods and time points, we randomly assigned patients in a double-blind setting and limited the study subjects to women who had undergone SPA-TLH. We performed an additional intergroup analysis based on time points, which quantified the severity of PONV based on NRS scores. While no significant difference in the incidence of PONV was found between the 2 groups at the 24- and 48-hour postoperative time points, a significant decrease in NRS score was observed between the experimental and control groups. The use of rescue antiemetics significantly decreased in the experimental group, which demonstrates that the administration of additional ramosetron was effective in reducing the incidence of PONV during the postoperative recovery period.
As with other types of selective 5-HT3 receptor antagonists, ramosetron has the potential to cause adverse effects. In our study, no significant difference in the reported adverse effects was found between the 2 groups. In the experimental group, headache occurred in 6 patients (13.3%) and dizziness occurred in 5 patients (11.1%), whereas in the control group, headache occurred in 5 patients (11.1%), dizziness occurred in 4 patients (8.9%), and constipation occurred in one patient (2.2%). No serious adverse effects were observed.
We limited the study subjects to patients who had undergone hysterectomy because they account for the largest population of patients who had undergone single-port laparoscopy-assisted gynecological surgeries. All the subjects were female, and most were middle-aged and premenopausal. Therefore, our results cannot be generalized to reflect a range of age groups. As no objective scoring system has been developed for nausea and vomiting, in this study, we used the NRS scoring system for evaluating the severity of PONV.
In conclusion, at 24 to 48 hours after SPA-TLH, a significant decrease in the severity of PONV (based on NRS scores) was found in the patients who were given additional prophylactic ramosetron as compared with the control group. A significant decrease was also observed in the additional use of rescue antiemetics in the experimental group as compared with the control group. Moreover, no severe adverse drug reaction occurred.
In addition to the conventional practice of administering a single dose of ramosetron immediately after surgery, based on our findings, the additional administration of ramosetron during the postoperative recovery period is recommended after laparoscopic gynecological surgery in patients at moderate to high risk of PONV.
Further studies should be performed to update the protocol for the administration of ramosetron for the prevention of PONV in patients who undergo SPA laparoscopic gynecological surgery.
 XML Download
XML Download