

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Persistent infection with the human papilloma virus (HPV) can cause malignant changes in the genital areas of men and women [1]. Human papilloma viruses (HPVs), responsible for causing cervical cancers, which affect a large number of individuals of the younger generation, also cause cancers of the vagina, vulva, penis, and anus, as well as infections of the head and neck region, conjunctiva, ear canals, nasal sinuses, and oral cavities [2]. After breast cancer, cervical cancer is the second most common cancer in the world among women, with a higher frequency of incidence and rate of mortality in developing countries than in developed countries [3].
Genotypes of HPV are divided into two categories—high-risk (HR-HPV) and low-risk (LR-HPV)-according to their ability to cause cancer [4]. LR-HPVs cause genital warts, and HR-HPVs cause abnormal cellular changes which progress to cancer in the cervix, vulva, and anus.
Majority (up to 90%) of newly acquired HPV infections similarly become undetectable within 1–2 years [5]. The HPV-DNA test is recommended for the detection of patients with infection in the latent period and that of HPV types. HPV-DNA detection is also necessary to produce effective vaccines. Women positive for the presence of HPV-DNA are considered to be infected and follow-up of HPV infections is based on HPV-DNA measurements at four, six, and twelve-month intervals [6].
Intensive studies on these viruses and their genotypes are being performed worldwide. The identification of commonly found genotypes in both, risk-patient groups, and in the general population is important for the prevention of HPV infection and for follow-up of associated diseases. Also, phylogenetic analyses and determination of the similarity of the HPV strains isolated from different regions help to clarify how viral genes and species develop, and which strains should be used for developing vaccines.
A study reported that more than 85% of the new HPV cases and HPV deaths occur in low-middle income countries [7]. According to the Republic of Turkey Ministry of Health data for 2016, Northeastern Anatolia, which includes Erzurum, is the region with the highest proportion (42.7%) of the rural population [8]. There are regional differences in terms of socio-cultural and economic levels of development in Turkey. Erzurum is located in a disadvantaged region due to high altitude of over 1,850 m and a terrestrial climate. Also, Erzurum shows poorer socio-economic development than the average of that seen in other parts of Turkey according to the development index [9]. In such a region, morbidity owing to HPV is expected to be high. Thus, we aimed to detect HPV-DNA positivity and to type and phylogenetically analyze isolated HPVs from smear samples taken from married women who visited the hospital for routine gynecological examination. Also, we wanted to report the first results for HPV genotypes for Turkey.
Materials and methods
1. Study group
This study was supported by the Atatürk University Scientific Research Projects Coordination Unit. The study included 263 married women who visited the Nene Hatun Maternity Hospital between April and December 2016 for routine gynecological examination. We selected cases from amongst women who had no history of malignancy. None of the women had a history of high-grade cervical intraepithelial neoplasia or cervical/vaginal/vulvar/anal cancer, or loop electrosurgical excision procedure conization treatment and hysterectomy. We provided detailed information to the patients about the procedure for collection of the cervical samples, and we provided them with questionnaires to complete in order to obtain their sociodemographic information and to determine their risk factors for HPV infection. Informed consent was obtained from all the women involved in the study.
2. Collection of specimens
Cervical smear specimens of patients applied to the hospital for gynecological examination were collected using a sterile speculum followed using a single-use sterile cervical brush which was rotated 360° clockwise in the cervical os. Samples were transferred to the Atatürk University Medical Faculty Molecular Microbiology Laboratory in sterile tubes along with the brush. In the lab, 1 mL sterile saline was added to the samples, and they were centrifuged at 3,500 rpm for 15 minutes. Then, fluids containing samples were transferred into Eppendorf tubes and were stored at −80°C in the freezer until DNA isolation was performed.
3. DNA isolation
A GF-1 Viral Nucleic Acid Extraction kit (Vivantis Technologies, Subang Jaya, Malaysia) was used to isolate viral DNA from cervical smear specimens. DNA isolation was performed according to the manufacturer's recommendations. First, 200 µL of the samples homogenized by vortexing were transferred to eppendorf tubes and 50 µL proteinase K was added to them. Then, 215 µL of Buffer VL containing Carrier RNA was added and mixed using pulsed-vortexing. This mixture was incubated at 65ºC for 10 minutes in the heating block. At the end of the incubation, 280 µL of absolute ethanol was added to each sample and samples were vortexed again. Samples transferred to filter tubes were centrifuged at 5,000 × g for 1 minute. Next, 500 µL of wash buffer 1 solution was added and samples were centrifuged at 5,000 × g for 1 minute. Wash buffer was added to the samples and they were centrifuged three times, twice for 1 minute each and once for 3 minutes at 5000 × g. Lastly, they were centrifuged at 5,000 × g for 1 minute. After each centrifugation, the remaining fraction was decanted. The nucleic acid suspensions thus obtained were maintained at -20°C until the polymerase chain reaction (PCR) assay was performed.
4. Polymerase chain reaction
In order to detect HPV-DNA, a PCR assay for the L1 gene region was performed. For this, the MY09/MY11 primer pair was used for the first round and then the GP5/GP6 primer pair for the second-round. The PCR reaction was carried out under conditions specified by Entiauspe et al. [10]. The primer sequences, target gene region, and amplicon sizes used for the study are shown in Table 1.
Table 1
Primers used in human papillomavirus screening and typing

The PCR mix used for the experiment was adjusted to a volume of 50 µL per sample. The PCR mix included reagents in the following amounts, PCR Master Mix 25 µL (Thermo scientific 2X PCR master mix, Life Technologies, Carlsbad, CA, USA); Forward primer (MY09/GP5) 1 µL; Reverse primer (MY11/GP6) 1 µL, ddH2O 17 µL, and 6 µL of template DNA were added to the reaction mixture. The ABI Data (Applied Biosystems, Foster City, CA, USA) thermal cycler was used for PCR. Amplification using primers HPV MY09/11 was performed as follows: 95ºC for 5 minutes, 40 cycles of 95ºC for 1 minute, 55ºC for 1 minute, 72ºC for 1 minute, ending with 72ºC for 10 minutes. Nested PCR was performed with the MY09/11 and GP5+/6+ primer sets. Amplification cycles were modified as follows: 95°C 5 minutes, 40 cycles of 94°C 30 seconds, 45°C 30 seconds, 72°C 30 seconds, ending with 72ºC for 10 minutes.
HPV-specific amplification products were visualized using a 1% agarose gel stained with ethidium bromide (Sigma-Chemical Co., St. Louis, MO, USA). Image evaluation was performed using the ultraviolet imaging system (Vilber-Lourmat, Collégien, France). The PCR-amplified HPV-positive amplicons were purified with the QIAquick PCR Purification kit (Qiagen, Hilden, Germany).
5. Sequencing and phylogenetic analysis
Sequence analysis was performed for forward and reverse sequences using purified HPV-positive DNA products and the MY09/MY11 primers. Sequence analysis was performed using the Sanger sequencing method and the BigDye Terminator v3.1 Cycle Sequence kit, using the ABI 3110xl DNA Analyzer (Applied Biosystems). Nucleotide sequences were evaluated using the Geospiza FinchTV program version 1.4.0 (Geospiza, Inc. Seattle, WA, USA). Our working samples and reference HPV-DNA sequences from the NCBI GenBank (http://www.ncbi.nlm.nih.gov/genbank/) were aligned using the BioEdit software package (v7.2.5).
6. Statistical analysis
Data are given in numbers and percentages. Statistical analyses were performed to determine the relationships between sociodemographic variables. The SPSS software (version 20.0, SPSS Inc., Chicago, IL, USA) was used for analyses. The χ2 test was used to determine statistical significance, P<0.05 was considered to be statistically significant.
Results
Voluntarily provided cervical smear specimens from 263 women who had no history of malignancy were investigated for the presence of HPV. Patients were provided with a questionnaire in order to obtain their socio-demographic information, in which they were required to provide their educational status, professional status, history of alcohol consumption, and history of sexually transmitted congenital syphilis or any other sexually transmitted diseases (STDs). The data are summarized in Table 2.
Table 2
Human papillomavirus (HPV) positivity in cases according to various demographic indications
The age group of the women enrolled for the study included women between 18–80 years, with an average age of 39 years, with a standard deviation of ±11.4 years. Majority of the cases belonged to the age group of 35–44 years; the highest HPV positivity was also seen in this group. HPV positivity increased rapidly from 18 to 44 years of age and decreased rapidly after the age of 45. However, the distribution of HPV positivity in the age groups did not show a statistically significant difference (P=0.66).
According to the results of the survey, seven women were employed, and the rest were housewives; except for one of the HPV positive women, the others were housewives. HPV positivity did not differ statistically according to the professional status of the subjects (P=0.39).
Majority of the women (85.9%) had completed education up to secondary school level or up to lower educational levels. The proportion of women with education from high school and above was only 14.1%. However, no statistically significant difference was found between education levels and HPV positivity (P=0.42).
None of the women had a history of alcohol consumption, thus, in our study, all HPV strains were isolated from women who did not consume alcohol. Thirty-five women (13.3%) were found to be habituated to cigarette smoking (from 2 to 40 cigarettes per day). Three of the HPV-positive cases were smokers; however, HPV positivity did not differ statistically between smokers and nonsmokers (P=0.48).
Two women had a history of STDs. One had a history of condyloma, whereas, the other woman's husband was affected with condyloma at the time of the study. However, the second woman was not included in the phylogenetic analysis, because sequence results from her samples were unclear. No statistically significant relationship was found between the presence of STDs and HPV positivity.
Seventeen HPV-positive samples were sequenced. Phylogenetic analysis was performed for 14, excluding 3 samples for which sequencing did not work well. Six of the typed samples were shown to be HPV 70 positive, four were HPV 16 positive, and the remaining four were HPV 54, 72, 81, and 114 positive. A total prevalence of 6.5% was found; of these, 1.5% were identified as HR-HPV and 3.8% as LR-HPV. Distribution of HPV types according to risk groups is shown in Table 3.
Table 3
Distribution of human papillomavirus (HPV) types according to risk groups

| Risk group | HPV types | No. (%) |
|---|---|---|
| LR-HPV | 54, 70, 72, 81, 114 | 10 (3.8) |
| HR-HPV | 16 | 4 (1.5) |
| Undefined HPV | - | 3 (1.1) |
| Total | - | 17 (6.5) |
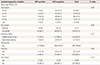
Fig. 1 shows the phylogenetic analysis of the L1 gene region in the HPV-DNA of the strains included in the study. Five genera, including Alpha, Beta, Gamma, Mu, and Nu, which cause human diseases, were included in the phylogenetic analysis. Reference genotypes obtained from the NCBI GenBank were used to construct the phylogenetic tree. The reference numbers of these strains were as follows: U45910, U45911, U45909, U45908, U45907, U45913, U45889, U44891, U45890, U45893, U45894, KT725857, KU298919, KU298928, EU918767, GQ244463, KC470249, KX514417, U21941, KU298914, HE574705, AJ620209, X94164, AF536179, HM596522, AF402678, AF472509, AF536180, DQ057331, DQ057332, DQ057330, DQ057327, KU298909, JX129488, M74117, KX514422, U45897, U45895, U45896, NC001457, X74464, NC001354, and U06714. Sequencing and phylogenetic analysis showed that all strains used for this study belonged to the genus Alphapapillomavirus affecting humans.
Fig. 1
Phylogenetic analysis of the L1 gene region in human papillomaviruses (HPV)-DNA positive specimens. HPVs classified in five different genera are indicated in the phylogenetic tree. All of our study samples in which the Alpha genus was included are shown with rounded black dots. Other examples mentioned in the phylogenetic tree were obtained from the National Center for Biotechnology Information (NCBI) GenBank and are shown by the access numbers.

Discussion
It is reported that the prevalence of HPV infection and HPV-induced disorders in Turkey is lower than that in many other developed countries, however, in recent years, the rates have increasing [11]. Bruni et al. [12] determined worldwide HPV prevalence which was found to be 11.7% in a meta-analysis study. In a study conducted in Thailand by Phoolcharoen et al. [13], highest HPV prevalence was seen in women between 20–30 years of age. Martins et al. [14] observed that the frequency of HPV infection decreased with increasing age in Brazilian women. In the multicenter study conducted in Turkey by Dursun et al. [15], highest HPV prevalence was detected in women under the age of 25, followed by that in the age group of 30–39 years, and then in women above 60 years of age. In our study, highest positivity of HPV-DNA was found in the 35–44 age group (9.2%) and the lowest positivity was found under 25 years (3.8%). These results are in contrast to those from other studies. It is not possible to comment on the low prevalence in the under-25 group, because the subjects were not asked to specify their age at the first instance of coitus and/or at the time of marriage for this study. However, we believe that the low HPV-DNA positivity in women under 25 years of age is probably related to the sexual habits of the women and their husbands, none of them have a history of malignancy and their lifestyles are modest.
Information about the prevalence of HPV obtained from a low-income population has been presented in this study, however, contrary to our expectation, the prevalence of HPV is low in Erzurum. Subjects enrolled for the study come from a conservative background, and they follow customs and are accustomed to reserved environment. Loyalty on part of both spouses is an essential part of our culture r. In addition, contraction of STDs is considered as dishonorable by the people of this region and hence, privacy of such cases poses an obstacle to sexual relations with multiple partners. Such a lifestyle and socio-cultural structure substantially prevents the risk of transmission of HPV. Men from this culture are circumcised according to tradition. Circumcision probably reduces HPV prevalence in Erzurum as well as in other provinces of Turkey. None of the subjects enrolled for the study are alcohol or substance addicts. We would like to emphasize that the most important factor in the low HPV prevalence found in our study is the absence of harmful urinogenital diseases in women.
The distribution of common HPV genotypes in the world varies from country to country. For example, the three most prevalent genotypes are 16, 31, and 6, found in Southern Italy [16]; 16, 51, and 52 in Thailand [13]; 58, 16, and 52 in Korea [17]; 53, 58, and 52 in Korea as found in a later study [18]; and 51, 11, and 16 in Qatar [19]. The most prevalent genotypes in provinces from different regions of Turkey are 16, 45, and 18 in Adana [20]; 18 and 16 in Konya [21]; 16, 11, and 6 in Ankara [22]; 16, 56, and 51 in Antalya [23]; 16, 18, and 33 in Elazig [24]; and 16, 18, 31, and 51 in Istanbul [25]. In our study, the most frequently seen genotypes were 70 and 16. Only one genotype was isolated among other genotypes including 54, 72, 81, and 114 found in our study. All other genotypes isolated in the study, apart from HPV 70, are frequently isolated in different regions of Turkey as well as in other countries. In this study, 1.5% of the identified genotypes were HR-HPV and the remaining (3.8%) were LR-HPV. Naturally, in our study, low-risk HPVs were detected at a higher prevalence than high-risk HPVs because subjects included in the study consisted of women who did not have malignant conditions such as high-grade cervical intraepithelial neoplasia, cervical/vaginal/vulvar/anal cancer.
HPV 70/85 is considered to be the HPV type of the highest mucosal oncogenic viral subdivision. Due to the close phylogenetic relationship with known carcinogenic types, this type has been introduced into the International Agency for Research on Cancer (IARC) category 2B, the category that includes carcinogens that affect humans [26]. HPV 70 is a genotype that can be isolated not only from women but also from genital warts of men [27]. We want to draw attention to the fact that this type of HPV has been reported for the first time in Turkey. HPV 81, 54 and 72 genotypes isolated in our study were also isolated in another study from Italy by Vergori et al. [28], from anal swab specimens of HIV-positive men. HPV114 was isolated from a low-grade cervical lesion by Ekström et al. [29] in Sweden.
It is most likely that, the differences in results obtained from our study according to the general profile of Turkey depends on the test method used, the number of samples, and preferences in sexual behavior of people living in the region. Although there are various studies that involve the identification and typing of HPV-DNA in cervical smear samples in the country, no large-scale study has been conducted for phylogenetic analysis of HPV. Phylogenetic analysis revealed the kinship grades of the strains obtained in our province using data from NCBI GenBank. The sequences of ERZ184, -134, -131, -115, -64 and -55 strains isolated in our study clustered with the Swedish HPV70 strain. ERZ25, -16, -12 and -10 isolated from this study clustered with the European (Greek and Germany) HPV16 strains, however, the Asian American variant and the American HPV16 strains clustered in a separate group. The strains ERZ190, -103, -202 and -142 isolated from our study clustered with strains from HPV 54 (Brazilian strain), HPV 72 (German strain), HPV 81 (German strain) and HPV 114 (Swedish strain), respectively.
Recently, a number of studies have been performed to determine phylogeny and nucleotide variability of multiple or single HPV types. In one of these studies, Aziz and colleagues found HPV 6, 55, 11, 43, 33, 18, 16 types in Pakistani women, and 80–99% nucleotide identity with types related to the same species of HPV. They reported that the sequences clustered with those from China, India, Mexico, Iran, Slovenia and Germany [30]. In China, Chen et al. [31] have isolated HPV 26, 51, 69, 82, 30, 53, 56, 66, 34, 73, 54 and 61, and they reported that heterogeneity and phylogeny of HPV isolates show an independent evolutionary history for each species. Cui et al. [32] reported that the E6 and E7 genes show nucleotide polymorphisms in some of the high-risk HPV45 strains identified in Southwest China. Conde-Ferraez et al. [33] reported that the E7 oncogene from the HPV type 58 was more conserved than the E6 gene in women from Southeast Mexico, and HPV 58 variants were not specific to a geographic region. Ramas et al. [34] reported that HPV16 variants isolated from Uruguayan women mostly clustered in the European lineage and a small part of them clustered in the Asian-American/North-American and African lineage, and additionally identified new variants in the European and African clusters. In China, Zhang et al. [35] identified mutation sites in the E5, E6, E7 and L1 genes of a significant proportion HPV 31 strains. These studies have shown that the distribution of HPV types in different countries is not affected to a great extent by geographical distances. Also, it emphasizes the importance of nucleotide polymorphisms and mutational changes in viral genes. In general, the magnitude of the prevalence of European HPV types in different countries, including Turkey, is noteworthy. So far, only one study has been conducted on the phylogenetic analysis of HPV genotypes in Turkey. In this study, Avci et al. [22] have performed a phylogenetic analysis of HPV 16, 11 and 6 detected in women with cervical pathologies from Ankara. However, it was not possible to compare our findings with this study as the details of phylogenetic characterization were not provided.
In conclusion, this study is the first study showing phylogenetic analysis and molecular characterization of circulating HPV types in married women over 18 years of age from the Eastern Anatolia Region of Turkey. In order to contribute to vaccine studies and to enrich the global HPV data, it is necessary to perform a greater number of such studies with larger sample sizes. The reason for the low rate of HR-HPV in our study is probably the fact that the subjects include women without malignant conditions. It is possible to say that their traditional and conservative lifestyle also contributes to the low rate of HR-HPV. Nonetheless, 1.5% women representing the normal population are at a risk of encountering HR-HPV strains.
 XML Download
XML Download