

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Gestational diabetes mellitus (GDM) is a common metabolic complication affecting 6–7% of pregnancies by western report [1]. Prevalence of GDM in Korea has increased from 1.7–3.9% in 1995 [2] to 3–5% in 2012 [3]. Of note, according to a recent Korean study using data from the Health Insurance Review and Assessment database showed that the prevalence of GDM in Korean women recently reached up to 5.7–9.5% between 2007 and 2011 [4].
It is well known that GDM patients are at higher maternal complications including gestational hypertension, preeclampsia, and increased cesarean section rate. Importantly, GDM is associated with increased risk of diabetes later in life. A Korean multicenter study including 1,686 patients recently reported that up to 18.4% of GDM was subsequently diagnosed as overt diabetes mellitus (DM) in postpartum period [5]. Fetal and neonatal complications of GDM include macrosomia, shoulder dystocia, neonatal hypoglycemia, neonatal respiratory distress syndrome (RDS) [16]. Although increased level of fasting blood glucose seems to be associated with higher risk of stillbirth during the last 4 to 8 weeks of gestation [6], the relationship between glycemic control and fetal death in the uterus is uncertain [7].
The recommended timing of delivery in GDM patients remains controversial. Whereas the American Diabetes Association recommends delivery during the 38th week of gestation [6], the American College of Obstetricians and Gynecologists guidelines suggest that well controlled patients without medication do not require delivery before 39 weeks of gestation. The timing of delivery in women with well controlled GDM by medical therapy is recommended from 39.0 weeks to 39.6 weeks of gestation [1]. In a randomized controlled trial on the induction versus expectant management of labor in GDM, the results showed no difference in pregnancy outcomes between the early induction group at 38 weeks of gestation and the expectant group up to 41 weeks of gestation [8]. However, for poorly controlled GDM patients, early delivery between 37.0 weeks and 38.6 weeks of gestation is supported [19]. Neonates of GDM patients have increased risks for RDS, low Apgar scores, admission to the neonatal intensive care unit (NICU) [10]. Delivery before 38 weeks of gestation can increase the risk of neonatal morbidity and mortality associated with prematurity. Delivery at later gestations poses neonatal risk of macrosomia, shoulder dystocia, and stillbirth, etc. Therefore, risk-based patient counseling is necessary as perinatal outcomes tend to differ according to the risk factors.
Several studies have been performed to find the associated factors of adverse prenatal outcomes in GDM patients. They included maternal obesity before conception, excessive weight gain, and HbA1c at diagnosis, etc. Since prenatal ultrasonography is frequently used to monitor fetal growth in GDM patients in obstetric practice, fetal biometric findings such as abdominal circumference (AC) could be readily utilized to assess the adverse outcome of neonates in GDM and are being incorporated in recent reports [11]. In fact, fetal ultrasound-guided therapy of GDM was already suggested to be used to limit excess macrosomia and large for gestational age (LGA) neonates [12].
With this background, the goal of this study was to perform a retrospective study to find out the clinical trend of Korean GDM patients over a 10-year period who delivered in our institution and to identify the risk factors of adverse outcomes among maternal baseline characteristics and fetal biometric parameters by prenatal ultrasonography.
Materials and methods
This is a retrospective cohort study by reviewing the electronic medical records of patients who delivered with the diagnosis of GDM between January 2006 and December 2015 at our institution, which is one of the tertiary hospitals located in Seoul, Korea. During the study period, 948 consecutive singleton pregnancies with GDM were identified. Pre-existing diabetes and multiple gestations were excluded in the research. All patients were diagnosed of GDM by the 2-step approach during pregnancy. Abnormal value for the 50 g oral glucose tolerance test (OGTT) was blood glucose ≥140 mg/dL. GDM was defined when 2 or more of the venous plasma glucose concentration equaled or exceeded the criteria at fasting, 1 hour, 2 hours, and 3 hours after 100 g oral glucose load. Abnormal values of the 100 g OGTT were defined as the fasting blood glucose ≥95 mg/dL, 1 hour blood glucose ≥180 mg/dL, 2 hours blood glucose ≥155 mg/dL, 3 hours blood glucose ≥140 mg/dL [6]. Women who were diagnosed of GDM underwent specialized GDM education program including diet and exercise details and were instructed about self-capillary glucose monitoring. After 1 or 2 weeks of glucose check, when the blood glucose did not meet the target level (fasting >95 mg/dL or 2 hours postprandial >140 mg/dL), insulin treatment was started with the supervision of physicians.
The composite adverse outcomes include macrosomia, shoulder dystocia, neonatal hypoglycemia, RDS, and admission to the NICU which occurred in term gestation. Macrosomia was defined as birthweight that equals or exceeds 4,000 g. Shoulder dystocia was defined as delivery requiring additional manipulation such as McRoberts' maneuver. Neonatal hypoglycemia was defined as the blood glucose <35 mg/dL at initial work up as previously used in other studies [13]. RDS was defined as presence of respiratory grunting and retraction of the chest, an increased oxygen requirement (FiO2 >0.4) combined with ground-glass appearance and air bronchograms on chest radiographs requiring surfactant treatment. Patients with sonographic results that were acquired less than 1 week before term delivery were selected to evaluate the relationship between sonographic findings and adverse outcomes. For fetal biometric findings, biparietal diameter (BPD), head circumference, AC, and femur length (FL) were collected.
At initial statistical analysis, we assessed whether the data followed a normal distribution. Most data showed non-parametric pattern except for HbA1c at delivery, and thus were reported as the median for continuous variables. The t-test (parametric variables) and the Mann-Whitney test (non-parametric) were used in the univariate analysis for continuous variables. The χ2 test (parametric) and Fisher's exact test (non-parametric) were performed for the categorical variables. First, characteristics according to 2 periods (between 2006 and 2010, 2011 and 2015) were compared. Second, variables which are related to adverse outcomes were evaluated in term deliveries by univariate analysis. Multivariate analysis was also used to identify factors that were associated most with adverse outcomes. Statistical analysis was conducted using SPSS (IBM, Chicago, IL, USA). A probability value of <0.05 was considered of statistical significance. The study was approved by the Institutional Review Board in Samsung Medical Center (No. 2017-08-094).
Results
Between January 2006 and December 2015, we identified 947 consecutive women with GDM who delivered in our institution. Since the total number of deliveries in our institution was 9,635 and 8,169 in period 1 and period 2, respectively, the incidence of GDM was calculated to be 3.9% in period 1 and 7.0% in period 2, showing an increasing trend. Maternal baseline characteristics of the study population according to 2 periods (period 1: 2006 and 2010, period 2: 2011 and 2015) are summarized in Table 1. Period 2 was associated with older maternal age (34 vs. 33, P<0.001) and higher proportion of primiparity (51.3% vs. 44.7%, P=0.046) compared to period 1. The proportion of GDM A2 was also higher (30.9% vs. 23.0%, P=0.009) in period 2 than in period 1. Although maternal body mass index (BMI) at pre-pregnancy was not different between 2 periods, BMI at delivery was significantly lower (25.7 kg/m2 vs. 26.6 kg/m2, P=0.010) in period 2, reflecting more strict maternal weight control. Comparison using BMI category showed similar results. The glucose levels from 50 g OGTT and 100 g OGTT were not different between 2 periods. HbA1c at diagnosis also showed no difference.
Table 1
Maternal baseline characteristics of gestational diabetes mellitus (GDM) by time period
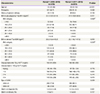
Values are presented as number (%), median (range), or mean±standard deviation.
BMI, body mass index; OGTT, oral glucose tolerance test.
a)Forty-six and eight patients were excluded from the analysis of BMI at pre-pregnancy and delivery respectively, due to unavailable information; b)By linear by linear analysis.
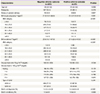
Table 2 demonstrated the delivery and neonatal outcomes of GDM in 2 periods. Overall, gestational age at delivery and the rate of preterm delivery showed no difference between 2 groups. As shown in Table 2, cesarean section rate (48.9% vs. 44.9%) and the rate of labor induction (27.0% vs. 30.4%) showed no difference in period 1 and period 2. Of note, the median neonatal weight at birth (3,110 g vs. 3,220 g, P=0.002) were significantly lower in period 2 compared to period 1. The composite adverse outcome, defined as any of macrosomia, shoulder dystocia, neonatal hypoglycemia, RDS, or admission to the NICU was not different between period 1 and period 2 (19.3% vs. 20.2%). Among adverse outcomes, RDS was significantly higher in period 2 compared to period 1 (6.8% vs. 3.5%, P=0.029). However, when limited in term birth, the incidence of RDS was similar in both periods (0.3% vs. 0.6%). The median neonatal glucose level was lower in period 2 compared to period 1 (65 mg/dL vs. 69 mg/dL, P=0.004). But the incidence of neonatal hypoglycemia showed no difference between 2 periods (3.0% vs. 2.5%). Similar findings were observed when limited to term birth group. That is, the median neonatal glucose level in term birth was lower in period 2 compared to period 1 (68 mg/dL vs. 71 mg/dL, P=0.028) but the incidence of neonatal hypoglycemia was similar between 2 periods (2.1% vs. 2.4%).
Table 2
Delivery and neonatal outcomes of gestational diabetes mellitus by time period
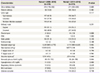
Since neonatal hypoglycemia and RDS among adverse outcomes were closely related with prematurity itself as well as GDM, we limited cases with term birth to identify risk factors for the development of adverse outcome of GDM in our study population. Among term birth, the incidence of shoulder dystocia, macrosomia, neonatal hypoglycemia, RDS, and admission to the NICU was 0.3%, 4.2%, 1.9%, 0.5%, and 2.9% respectively. Maternal characteristics according to adverse outcomes among patients who delivered at term are summarized in Table 3. The median maternal pre-pregnancy BMI (23.4 kg/m2 vs. 21.8 kg/m2, P=0.001), maternal BMI at delivery (27.9 kg/m2 vs. 25.8 kg/m2, P<0.001), HbA1c at diagnosis (5.6% vs. 5.3%, P<0.001), and mean HbA1c at delivery (5.8% vs. 5.5%, P=0.044) were significantly higher in the group with adverse outcomes. Among patients who delivered at term, only patients with prenatal ultrasonography results achieved less than one week before delivery were selected to undergo analysis to find relationships between sonographic results and adverse outcomes. As shown in Table 4, the AC, the percentile of AC, estimated fetal weight (EFW), and the percentile of EFW manifested significantly larger in the adverse outcome group.
Table 3
Comparison of maternal characteristics according to adverse outcome in term pregnancy
Values are presented as number (%), median (range), or mean ± standard deviation.
BMI, body mass index; OGTT, oral glucose tolerance test; GDM, gestational diabetes mellitus.
a)Fifteen and three patients were excluded from the analysis of BMI at pre-pregnancy and delivery, respectively, due to unavailable information.
Table 4
Comparison of ultrasound findings according to adverse outcome in term pregnancya)

BPD, biparietal diameter; HC, head circumference; AC, abdominal circumference; FL, femur length; EFW, estimated fetal weight.
a)Among term pregnancies, only patients whose ultrasonography results achieved in less than one week before delivery were selected for statistical analysis; b)Based on the report from National Data from Korean Health Insurance Review and Assessment Service 2009; c)Based on the study by Hadlock FP, Deter RL, Harrist RB, Park SK. Estimating fetal age: computer-assisted analysis of multiple fetal growth parameters. Radiology 1984;152:497-501.
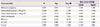
Lastly, since each parameter related to adverse outcome found by univariate analysis is closely interrelated, we performed a multivariate analysis to identify independent risk factors for the development of adverse outcome in term birth. Among the variables that were statistically significant in the univariate analysis, we went through linear regression to discard variables that showed multicollinearity. We selected 8 variables according to statistical or clinical significance. The variance inflation factor of each variable was low enough to move on to the multivariate analysis. Maternal pre-pregnancy BMI, fasting blood glucose at 100 g glucose tolerance test (GTT), 3 hours blood glucose at 100 g GTT, HbA1c at diagnosis, fetal BPD, fetal AC, and the fetal FL were included in the multivariate analysis after considering multicollinearity of each parameter. As shown in Table 5, Multivariate analysis showed that pre-pregnancy BMI (odds ratio [OR], 1.101; 90% confidence interval [CI], 1.028–1.180) and the fetal AC (OR, 1.218; 90% CI, 1.012–1.466) were the risk factors associated with the development of adverse outcome composed of shoulder dystocia, neonatal macrosomia, neonatal hypoglycemia, RDS, and admission to the NICU in term birth.
Table 5
Multivariate analysis of risk factors associated with adverse outcomes
Discussion
Our study demonstrated that the median age of GDM patients over recent 10 years has increased from 33 between 2006 and 2010 to 35 between 2011 and 2015. This trend obviously reflects our well-known national phenomenon of increased maternal age at childbearing in Korea. For example, mean maternal age was 30.4 years in 2006 and 32.2 years in 2015, respectively, as reported by Korean statistics [14]. And it also implies that older maternal age is associated with the development of GDM. Mean maternal age of our study population is slightly older than another report studying 1,161 GDM patients between 2006 and 2011 in which the mean age was 32 [15]. Our study also indicated that the requirement for insulin has increased from 23.0% between 2006 and 2010 to 30.9% between 2011 and 2015 among GDM patients. These proportions of GDM A2 among our study population are much higher than that from national data showing 5.94% to 13.87% (study period 2007 to 2010) of GDM cases requiring insulin treatment [16], obviously reflecting more high risk GDM in our hospital.
Nowadays, the importance of strict glucose control in GDM is well recognized both by patients and physicians. Our data provided the actual incidence of adverse outcome with contemporary standard care of GDM in a tertiary center. In assessing adverse outcomes, we excluded preterm birth since neonatal hypoglycemia and RDS are more closely connected to prematurity rather than glucose intolerance. Accordingly, among term birth, the actual incidence of shoulder dystocia, macrosomia, neonatal hypoglycemia, RDS, and admission to the NICU was 0.3%, 4.2%, 1.9%, 0.5%, and 2.9%, respectively, with a relatively low frequency. Therefore, in this study, we defined adverse outcomes as a composite of shoulder dystocia, neonatal macrosomia, hypoglycemia, RDS, and admission to the NICU. The incidence of such outcome was 11.6% among term birth. So, this number can provide useful and practical information in counseling GDM patients in the future.
In fact, our observation that the adverse outcome in GDM patients was associated with increased maternal BMI at pre-pregnancy or delivery, higher HbA1c at diagnosis or delivery by univariate analysis is not a new finding. Abundant studies have assessed the risk factors for the development of adverse pregnancy outcome (APO) in GDM as well as gestational impaired glucose tolerance [17]. Our study is in line with previous studies reporting that pre-pregnancy BMI is associated with APOs [1819]. A recent Korean study including 306 GDM patients in a single tertiary center also indicated that higher BMI at entry and fasting blood glucose are significantly associated with adverse outcomes (defined as neonatal hypoglycemia, hyperbilirubinemia, and hyperinsulinemia; admission to the NICU; LGA; gestational insulin therapy; and gestational hypertension) [20]. Pre-pregnancy BMI is one of the most important clinical variables of GDM since it can be corrected to prevent APOs [21].
Importantly, our data indicated that, following the known risk factor of pre-pregnancy BMI, fetal AC is the most independent variable associated with the adverse outcome that is defined as a composite of macrosomia, shoulder dystocia, neonatal hypoglycemia, RDS, and admission to the NICU in term gestation. In fact, fetal growth-based strategy to guide management of gestational diabetes was previously explored by another study [22]. It was also reported that fetal AC correlated well with fluctuating glycemic control [23]. However, none of other studies directly used fetal biometric findings obtained before delivery nor integrated them with maternal clinical characteristics including BMI at pre-pregnancy or delivery to elucidate the relationship between fetal biometric findings and adverse outcomes by multivariate analysis. Meanwhile, risk factors used in our study is closely inter-related with each other, and the interpretation of this study is not intended to disregard the risk factors which were meaningful by univariate analysis but to disclose that fetal AC is the independent risk factor associated with adverse outcome of GDM.
Notably, when we defined GDM as first recognition during pregnancy, there were 992 GDM cases and about 10.1% of this study population showed glucose level that equals or exceeds 200 mg/dL in 50 g OGTT which, along with symptoms such as polydipsia or polyuria, is suggestive of DM [24]. In fact, by several authors, the upper cutoff value of 50 g OGTT to omit further diagnostic test was reported to range from 220 mg/dL to 230 mg/dL [2526]. Our group also previously indicated that glucose level above 228 mg/dL from 50 g OGTT showed 100% positive predictive value for the presence of GDM [27]. Furthermore, 2.2% of these first recognized GDM patients manifested fasting glucose level that equals or exceeds 126 mg/dL in 100 g OGTT, in which the presence of overt DM is also highly suspected [24]. This proportion of patients may represent undiagnosed overt DM although GDM is usually defined as glucose intolerance with onset or first recognition during pregnancy [28].
There may be some limitations in this study. First, we used self-reported pre-pregnancy weight in cases where the diagnosis of pregnancy was made in another hospital. Second, although this study includes a large sample size it contains only patients from a single tertiary hospital and thus cannot represent the total Korean population. Despite the limitations listed above, there are strengths to this study. This study includes a large sample size and the patients all received a consistent diagnosis, antenatal and perinatal care in a single tertiary center. This can provide practical information for obstetricians counseling and managing GDM women.
 XML Download
XML Download