

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
There is a recommendation by the American College of Obstetricians and Gynecologists and the Royal College of Obstetricians and Gynaecologists (RCOG) that decision-to-delivery interval (DDI) in emergency cesarean delivery should be within 30 minutes [12]. The 30-minute rule was granted by the consensus of experts without acknowledges supporting study. No evidence has been found to prove that the 30-minute rule helps improve maternal or fetal outcomes [3]. Furthermore, DDI of 30 minutes is difficult to achieve in many settings according to various problems in real clinical practice [456].
The latest RCOG National Institute for Health and Care Excellence (NICE) guideline has recommended that category 1 (immediate threat to life of the woman or fetus) and category 2 (maternal or fetal compromise that is not immediately life-threatening) cesarean sections should be carried out within 30 minutes and 75 minutes after the decision, respectively. They also recommend the use of 30-minute and both 30- and 75-minute intervals to measure the overall performance of an obstetric unit in category 1 and category 2 cesarean sections, respectively [7].
Many factors have been reported to affect DDI, including team readiness, team communication, availability of operating room and severity of fetal-maternal complications [8]. Previous studies reported that good preparation can reduce DDI, such as locating operating room near delivery room, availability of obstetricians and anesthesiologists, and an effective teamwork. In developed countries, achievement of 30-minute goal as recommended among cases diagnosed with fetal distress was approximately 40%–65% [56910]. Meanwhile, in developing countries, the achievement has been reported to be only 0%–20% [111213].
In Thailand, there is limited information regarding the time interval for emergency cesarean delivery and no specific recommendation has been adopted. A recent report in Thailand showed that only 6.6% of women with non-reassuring fetal heart rate (FHR) pattern achieved the 30-minute goal for cesarean delivery with a median time of 56 minutes [14]. However, such study focused on only women with non-reassuring FHR, but not on women with other indications for emergency cesarean delivery. Exploring and understanding of the time process of emergency cesarean delivery in real clinical practice would provide more insight into the appropriateness of current management protocols and related information on the delay. In addition, it would also help in providing further information related to medico-legal claims in general obstetric practice.
Therefore, the primary objective of this study was to determine the DDI for emergency cesarean delivery. Adverse perinatal outcomes, potential associated factors, and the time intervals of care processes were also evaluated. The results can be regarded as an audit and subjective evaluation of performance of current management provided to this group of women in the institution. The information would also guide the care team to identify the cause of the delay and its barriers with firm evidence in order to improve the quality of care given to these patients. The findings will provide additional information for other settings with similar care problems and processes at both national and international levels. Moreover, policy makers can also use this information to plan future improvements in the patient care process for better care of pregnant women.
Materials and methods
After approval by the Siriraj Institutional Review Board, this retrospective cohort study was conducted at the Department of Obstetrics and Gynaecology, Faculty of Medicine Siriraj Hospital, which is the largest University-based tertiary referral center in Thailand. After informed consent, a total of 431 term, singleton pregnant women who were indicated for emergency cesarean delivery were included during January to April 2016. Women with detected fetal anomalies and intrauterine fetal death were excluded. During labor, all of the women were managed according to institutional clinical protocol. Decision for emergency cesarean delivery was made by attending staff based on available clinical information on a patient-by-patient basis. The anesthetic methods for cesarean delivery were determined by the attending anesthesiologist.
The data were obtained from medical records, including baseline characteristics, obstetric data, antenatal and intrapartum characteristics, indication for cesarean delivery, and neonatal outcomes. The component process times from decision-to-delivery were recorded and reviewed, including time of decision, time of entering the operating room, time of skin incision, and time of delivery. The decision time was also classified as having been made either during or after normal office hours. According to the NICE recommended guideline and to further facilitate the analysis, DDIs were classified into the following 3 groups: ≤30, 31–75, and >75 minutes [7].
Descriptive statistics, including the mean, standard deviation, median, interquartile range, number and percentage were applied as appropriate. Comparisons between and among groups were performed using Student's t-test, Mann-Whitney U test, χ2 test, Kruskal-Wallis test, and analysis of variance as appropriate. Subgroup analysis was also performed using factors that potentially affected time intervals. P-values less than 0.05 were regarded as being statistically significant. All statistical analyses were performed using IBM® SPSS® Statistics version 21 (IBM Corp., Armonk, NY, USA).
Results
During January to April 2016, there were 1,418 deliveries and 559 were cesarean deliveries (39.4%). Indications for cesarean delivery included previous cesarean delivery (13.3%), cephalopelvic disproportion (CPD; 8.9%), non-reassuring FHR (6%), and others (11.2%). A total of 431 women underwent emergency cesarean delivery were included. Table 1 shows baseline characteristics of the participants. The mean maternal age was 30.4±6.1 years, and the majority of patients were nulliparous (59.4%). The mean gestational age at delivery was 37.9±2.1 weeks. The most common indication for emergency cesarean delivery were CPD (27.4%). Non-reassuring FHR was found in 14.8% and only 6 cases (1.4%) were in category III according to the National Institute of Child Health and Human Development (NICHD) classification. One-third (33.2%) of the operations were performed during office hours. The majority of operations (90.7%) were done under regional anesthesia.
Table 1
Baseline clinical characteristics of the study population (n=431)

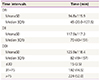
The intervals from decision for cesarean delivery to various endpoints was shown in Table 2. The median time for decision-to-operating room interval (DRI), decision-to-incision interval (DII), and DDI were 45, 70, and 82 minutes, respectively. Only 3.5% of cases had DDI of ≤30 minutes, while as many as 52.0% had DDI of >75 minutes.
Table 2
Intervals from decision for cesarean delivery to various endpoints (n=431)
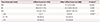
Comparisons of various process intervals between different decision time was shown in Table 3. Compared with operation performed during normal office hours, every time interval was significantly shorter during after office hours (DRI: 70.0 vs. 37.5 minutes, P<0.001; DII: 96.0 vs. 62.5 minutes, P=0.001; and DDI: 103.0 vs. 69.0 minutes, P=0.001). DDI of ≤30 minutes were achieved in 4.9% of cases during after office hours compared to only 0.7% during normal office hours (P=0.001), and DDI of >75 minutes was also significantly lower (45.8% vs. 64.3%).
Table 3
Comparison between intervals from decision to various endpoints between different decision time
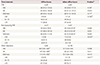
When stratified by indications for cesarean delivery, every time interval in the patients with non-reassuring FHR was significantly shorter than those with CPD and other indications, as demonstrated in Table 4. DDI of ≤30 minutes was achieved in 18.8% of those with non-reassuring FHR while it was only 0.8% among those with other indications (P<0.001).
Table 4
Comparison between intervals from decision to various endpoints between different indication for cesarean delivery

Values are shown as median (IQR) or number (%).
DRI, decision-to-operating room interval; DII, decision-to-incision interval; DDI, decision-to-delivery interval; CPD, cephalopelvic disproportion; FHR, fetal heart rate; IQR, interquartile range.
a)Kruskal-Wallis test; b) Significantly different compared to other indications; c)Significantly different compared to CPD and others indications; d)χ2 test.
Comparisons of intervals from decision to various endpoints among different decision times and indications for cesarean delivery were outlined in Table 5. In terms of DDI, the best performance was observed among non-reassuring FHR pattern during after office hours, and worst performance was observed among those with other indications during normal office hours. A significant shorter DDI was observed during after office hours in those with non-reassuring FHR and other indications, but not CPD. For non-reassuring FHR pattern, 23.4% had DDI ≤30 minutes during after office hours, compared to 5.8% during office hours (P=0.032), with the median DDI of 45 and 64 minutes, respectively (P=0.042).
Table 5
Comparison between intervals from decision to various endpoints between different decision time and indication for cesarean delivery
Values are shown as median (IQR) or number (%).
CPD, cephalopelvic disproportion; DRI, decision-to-operating room interval; DII, decision-to-incision interval; DDI, decision-to-delivery interval; FHR, fetal heart rate; IQR, interquartile range.
a)Mann-Whitney U test; b)χ2 test; c)Significantly different from CPD and other indications during after office hours; d)Significantly different from CPD and non-reassuring FHR during office hours.
Neonatal outcomes were compared between the 3 DDI categories and are shown in Table 6. No significant differences were observed among groups in terms of birth weight, birth asphyxia, or neonatal intensive care unit admission. Other complications including respiratory distress, transient tachypnea of the newborn, meconium aspiration, and sepsis were also comparable between groups.
Table 6
Comparison of neonatal outcomes between various decision-to-delivery intervals

Discussion
The results of this study demonstrated that the median DDI among patients with emergency cesarean delivery was 82 minutes, and only 3.5% has DDI ≤30 minutes. This is corresponded to previous studies that DDI was commonly longer than the 30-minute recommendation in real clinical practice, especially among developing countries [45610111213]. However, the results also showed that 48% had DDI ≤75 minutes, which is the suggested time for non-life-threatening cesarean delivery [7].
Since the 30-minute goal has been advocated, no scientific evidence supports this threshold that DDI ≤30 minutes could improve perinatal outcome [38]. The latest Guidelines for Perinatal Care refers only to an obstetric unit's capability to respond to an obstetric emergency, with no mention about requirements for delivery within any time frame [15]. It was recommended that DDI should be based on the timing that best incorporates maternal and fetal risks and benefits and should be tailored to local circumstances and logistical capabilities. The NICE guideline has been using 30- and 75-minute rules only for clinical audit of the quality of hospitals and not judging multidisciplinary team performance for any individual cesarean delivery [7].
Many factors play an important role in achieving the 30-minute goal, including the obstetric care unit setting, availability of operating room, the clinician's perception of delivery urgency, severity of fetal-maternal complications, and the communication and transfer processes of the setting [816]. In this study, component time intervals and factors potentially affecting the DDI were evaluated, including the decision time and indication for cesarean delivery (which partly reflects the level of emergency). The results demonstrated that the median DRI contributed mainly for DDI. In addition, when the decision was made after office hours, every time process was significantly shorter than during office hours. Median DRI was only half of office-hour cases (37.5 vs. 70 minutes), median DDI was reduced to 69 minutes, 4.9% achieved the 30-minute goal, and more than half (54.2%) had DDI ≤75 minutes. Similar better performance during after office hours was observed in every indication of cesarean delivery. This reflected that patient transfer process, as well as availability of operating room are important factors for DDI [517].
Similar to other studies, another factor influencing DDI is the severity of maternal and fetal conditions, as specified by indication for cesarean delivery [818]. Significant shorter time intervals were observed among those with non-reassuring FHR pattern that median DDI was 47 minutes and 18.8% and 75% had DDI ≤30 and <75 minutes, respectively. Similar significant shorter DDI was also observed even among cases after office hours. This might be due to an increased sense of awareness from the level of emergency among these cases.
However, it should be noted that, among non-reassuring FHR cases, there was still an average of 20 minutes difference between room-in and incision time. This was probably due to the combination of process of patient preparation, anesthesia, and degree of abnormal FHR. In this study, majority of women with non-reassuring FHR pattern were in NICHD category II that regional anesthesia was provided. On the other hand, the other 6 cases with abnormal FHR in NICHD category III which immediate delivery was required, general anesthesia was provided and the median room-in to incision time was reduced to 10 minutes.
Previous studies reported an improvement in the time to delivery by implementing a multidisciplinary protocol, a team training with more effective communication and an obstetric care process [1920]. The results of this study also showed some improvement in the care process among women with non-reassuring FHR, compared to a recent report from the same institution [14]. Achievement of 30-minute goal increased from 6.6% to 18.8% and rate of delivery in ≤75 minutes increased from 69.5% to 75%. The median DDI has been improved from 56 to 47 minutes. This was partly due to an improvement in care process, team communication, and guideline amendment that were implemented after the results of previous study.
No significant differences in perinatal outcomes between various DDI was observed in this study. Similar results were reported in previous studies [8913182122]. However, a previous study showed that DDI >75 minutes was significantly related with poor perinatal outcomes such as asphyxia and increased in the need for special care [23]. Another study also reported a significant improvement in neonatal outcomes after the DDI in emergency cesarean delivery was shortened, especially in severe irreversible indications such as cord prolapse and placental abruption [20].
Some limitations of this study need to be addressed. The evaluation of the actual cause of delays (e.g., transfer process details, availability of operating room at decision time, anesthetic difficulty) was not possible due to the retrospective nature of this study. In addition, limited sample size in subgroup analyses might result in insufficient power to detect significant differences between groups. Larger prospective studies should be conducted to determine the DDI in various specific subgroups and to evaluate the actual causes of delay in details.
It is recommended that all obstetric unit should improve the time to delivery by realizing the process of emergency cesarean delivery. Communication skills and team readiness should be improved, either by team training and regular audit [19]. Prioritization by the severity of various indications should also be considered. The operating room should always be available for emergency cesarean deliveries especially for extremely urgent indications.
Although the results are similar to those of other previous reports, these findings provide additional information for both local and national policy makers to plan future improvements in the patient care process. Moreover, the results could be shared with other settings with similar care problems and processes. Nonetheless, further continuous quality improvement processes should be developed and implemented. Processes between decision and delivery should be evaluated systematically and in more details to determine possible barriers and appropriate solutions.
In conclusion, only 3.5% of emergency cesarean delivery had a DDI ≤30 minutes (median 82 minutes). Significant shorter time intervals were observed in those with non-FHR pattern and when the decision was made after office hours. Causes of the delay should be further investigated and continuous quality improvement in the care process is warranted in order to minimize the unnecessary delay and improve maternal and neonatal outcomes.
 XML Download
XML Download