

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Hysteroscopic sterilization (HS) first appeared on the US market in 2002 when the Essure device (Bayer Corp., Whippany, NJ, USA) gained approval by the US Food and Drug Administration. It remains the only available hysteroscopic contraceptive method in the US. The procedure does not require general anesthesia, involves no incision, and may be completed in as a little as ten minutes [12]. As background, HS involves placing a pair of small, flexible inserts consisting of nickel-titanium and polyethylene terephthalate (PET) fibers through the fallopian tubal ostia via a transcervical approach. The devices trigger an intraluminal inflammatory reaction resulting in tubal fibrosis and eventual occlusion. While HS has enjoyed considerable popularity, various complications have been described in the medical literature [345] and reported to health regulators [6]. Fortunately, removal of HS devices has been shown to resolve symptoms for many patients [78]. While there is no consensus on a preferred method to remove Essure implants, hysterectomy has emerged as one way surgeons can manage Essure complications [58910]. The relation between Essure and subsequent operation (including hysterectomy) has not been closely studied, however.
After cesarean delivery, hysterectomy is the most frequently performed surgery for women in the US [11] and accurate data regarding indications for this operation informs a crucial part of monitoring health outcomes. Most estimates of national hysterectomy activity cannot offer a comprehensive assessment because registries are generally restricted to surgeries performed in formal hospital settings [12]. Likewise, a major data gap also exists with respect to HS because there is no national registry for this procedure and many patients obtain Essure in doctor's offices or ambulatory surgery centers. Statistical impairments thus exist both for HS and hysterectomy, as reliance on standard hospital reports necessarily fails to capture the full picture for either of these events.
Researchers interested in hysterectomy have attempted to tackle this problem by adjusting their study design to follow insurance payments instead of hospital-level data [11]. Unfortunately, such an approach is unlikely to sharpen our understanding of HS, since although this elective sterilization technique is often done on an out-patient basis, it is not uniformly covered by insurance plans in the US [131415]. Of note, not even the device manufacturer knows how many women have had the HS procedure (in the US or elsewhere) and only data on the approximate number of Essure kits sold has been provided to regulators [16]. Thus, measuring any overlap between HS and hysterectomy—both gynecological interventions with substantial lifestyle implications—is an extremely difficult task.
Against this background, ours is the first investigation to present patient-level data to describe which operations are performed as a consequence of HS-associated symptoms. We were also interested in gathering basic information on patient age both at time of their elective sterilization with Essure, and at time of their subsequent surgery.
Materials and methods
A questionnaire was developed specifically for women who had HS followed by device removal surgery performed later specifically for new symptoms developing subsequent to Essure placement. Queries did not collect any personally identifiable information, were structured to permit numerical or text responses (Table 1), and then configured for an internet interface. For this study, any removal of the uterine corpus and fallopian tubes (with or without oophorectomy) as a method to manage post-HS symptoms was classified as hysterectomy. “Device removal only” surgery was defined as laparotomy or laparoscopy performed to excise Essure devices without hysterectomy, such as by salpingectomy. In the absence of a nationwide HS patient registry or unique International Classification of Diseases (ICD)-9/10 codes which could be used to filter for specific conditions associated with Essure, intake for this study was open to patient volunteers registered with an online education and advocacy group (“Essure Problems”, n=29,923). This represents the world's largest internet resource for Essure patients (https://www.facebook.com/groups/Essureproblems/). The research questionnaire was posted in English and remained active from July 2014 to February 2016. Incomplete questionnaires were excluded and responses were electronically tracked to block duplicate submissions from the same individual (via birth month/year entry and IP address tracking). An independent institutional review board considered the study prior to questionnaire launch and the protocol was judged as “no risk to human subjects” and exempted from review as the study involved no direct patient contact and data were processed in an anonymous, non-identifiable manner.
To validate self-reports, a review was performed on a subset of respondents (n=297) to confirm 1) that HS had been performed and document the date of the Essure procedure, and 2) that a formal operative note agreed with the subsequent (post-HS) procedure described by the patient. Subset analysis was completed by matching pathology reports/operative notes with corresponding survey responses, and all documents were immediately redacted after collation to protect patient confidentiality. Only investigators had access to running totals of the questionnaire during the study, and none of the investigators were physicians involved in Essure placement or device removal for any study participant. Although subjects were required to register via computer to access the questionnaire site, there was no cost to do so and respondents received nothing of value in exchange for their responses.
Patient data were analyzed with Python ver. 2.7.11 and the SciPy ver. 0.17.1 package (Enthought, Austin, TX, USA). For normally distributed data (i.e., patient age), mean and standard deviation were used to describe data location and dispersion. The Welch two sample t-test was used for comparisons of normally distributed sample means. For non-normal data (i.e., HS to subsequent surgery interval), median and interquartile range (IQR) were calculated. The Mann-Whitney U-test was applied for comparisons of two sample locations from non-normal data. For percent comparisons from one sample, the Student's t-test was used. By default, confidence level was set at 95% for all analysis.
Results
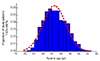
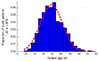
For this investigation, 3,803 voluntary patient reports were obtained from women who had undergone HS and had at least one other subsequent operation attributed to problems with the Essure device. Mean±standard deviation (SD) age for the overall study population was 35.6±6.3 years. The earliest HS event in this sample occurred in November 2002 and the most recent HS was December 2015. Among HS patients in this group, mean±SD age at time of the Essure procedure was 31.7±6 years. Clinical and demographic characteristics of the study population are summarized in Table 2. With regard to gynecological procedures performed after HS (Fig. 1), women having hysterectomy after Essure placement comprised 64.9% of patients in this series (n=2,468). For these patients, the median interval between HS and hysterectomy was 3.7 (IQR, 3.9) years and mean age at time of hysterectomy was 36.3±6.3 years (Fig. 2).
Other patients sought non-hysterectomy removal of HS devices (e.g., bilateral salpingectomy). For these women (n=1,035), mean interval between the Essure procedure and device removal was 3.1 (IQR, 4.0) years and mean patient age at time of device removal was 34.5±6.2 years.
Our analysis also identified a subset of women who underwent “other procedures” after Essure. For these patients (n=300), neither salpingectomy nor hysterectomy was performed after HS but instead dilation & curettage (n=229), endometrial ablation (n=202), hysteroscopy only (n=30), or diagnostic laparoscopy (n=16) was completed either alone or in combination. For patients in this group, mean interval between the Essure procedure and subsequent procedure(s) was 3.0 (IQR, 3.8) years. Age at time of second surgery was 34.1±6.0 years in this group.
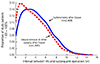
As summarized in Fig. 3, when all data from patients who had any post-Essure surgery besides hysterectomy were aggregated (e.g., device removal plus all “other” cases, n=1,335) and compared to those cases undergoing hysterectomy, mean±SD age was substantially lower than the group undergoing hysterectomy (34.4±6.2 vs. 36.3±6.3 years, respectively; P<0.01). Moreover, examination of the interval to surgery following HS found that hysterectomies were performed a median of 3.7 years after Essure, while uterus-conserving surgeries were typically performed significantly earlier (Fig. 4).
Because patient birthdate and the timing of HS and subsequent surgery were both tabulated, it was also possible to calculate patient age at time of Essure procedure as a function of which surgery type occurred later. From this, we found that patients who eventually underwent hysterectomy were significantly older for their Essure procedure compared to patients who had device removal only or other post-HS procedures (Table 2).
Discussion
There appears to be no clear consensus on how best to manage Essure patients who subsequently develop symptoms associated with HS [17]. While the notion that Essure patients might require further surgery is not entirely new, at least for the population of Essure patients sampled here the reliance on hysterectomy was higher than expected. For example, a mixed-model accounting cluster analysis evaluated 30-day and 1-year outcomes after >8,000 Essure procedures in New York State and found the risk of undergoing reoperation was more than 10 times higher for HS patients compared to patients undergoing standard laparoscopic tubal ligation [18]. Our work refines this observation by contributing a more detailed understanding of surgeries performed on Essure patients, as well as when they occur.
As HS coils are intended to be permanent contraceptive implants, it is not surprising that familiarity with their surgical excision remains limited [5819]. It is encouraging that satisfactory relief of Essure-associated symptoms has been reported as soon as two weeks following removal [20]. The current study captures more than a decade of HS experience, and is the first to show that the predominant surgical answer to Essure complications appears to be hysterectomy for many women. Moreover, the finding that hysterectomy occurs for Essure patients at about age 36 represents an original contribution to the contraceptive literature.
Why might HS be perceived as superior to traditional bilateral tubal ligation? A 2009 decision tree analysis to estimate procedure costs is sometimes cited to support the position that HS brings a cost advantage over standard tubal sterilization [21]. Such a model now seems problematic as it incorrectly assumed that patient satisfaction would be similar between the two comparator groups. Because few patients in HS premarketing studies were followed for more than 12 months [22], how many might seek additional surgery to “undo” Essure after the first year of use could not have been known previously. Although it is not surprising that such extra surgery brings additional expense, some research has shown that a priori costs for HS are already higher than for laparoscopic tubal ligation despite shorter operative time and less frequent use of general anesthesia [18]. Controversy also exists concerning the effectiveness of HS as a method of reliable birth control [2324]. This raises the question of device failure with profound economic and social implications of its own [25]. While none of this information was available for consideration when Essure was initially approved by the US Food and Drug Administration in 2002, awareness of such factors now could explain the level of patient interest in surgical device removal.
Likewise, hysterectomy may be perceived (either by physicians, patients, or both) as superior to other less invasive surgical approaches for Essure abatement—a related topic requiring cross-disciplinary study. For example, it is possible that the lack of a current procedural terminology code specific to surgical Essure removal favors hysterectomy, a surgery for which multiple current procedural terminology codes exist. Despite the known higher cost, intraoperative blood loss, overall complication rate and increased recovery time associated with hysterectomy, this surgery could nevertheless be preferred over less aggressive operations for which insurance companies might reject or delay the claim (i.e., no timely disbursement).
This study has several limitations which should be recognized. Interpreting HS data continues to frustrate regulators, patients, and advocacy groups; this lack of comprehensive reporting on Essure was equally vexing for our research. There is no agreement on the exact Essure complication rate, and until the regulatory climate changes to enable acquisition of HS data with greater precision, internet-based assessment tools (like the one we used) may supply the best available evidence on HS. Accordingly, we did not attempt to calculate reoperation rates from these data, but rather sought to enumerate which surgeries were performed among women in a self-selected group. Although it would have been ideal to have data provided by institutional sources, because authentication was achieved by a representative subsample audit the reliability of our information can be considered robust. Similar patient-completed surveys have been used in previous pelvic surgery contexts with good results [2627]. There is also the matter of linking HS to whatever operation which followed, and determining what factors (physician and/or patient) resulted in particular post-HS interventions. We were unable to evaluate the presentation of patients directly, therefore any clinical factors influencing selection of certain surgeries after HS cannot be known (e.g., data on body mass index, smoking status, medical history, or other comorbidities were not available for review). Like much of the Essure phenomenon, however, this is an underdeveloped area of inquiry awaiting additional research for clarification. The lack of established clinical guidelines for Essure removal appears to permit a considerable range of surgical approaches in routine practice.
For many women, their contraceptive journey with Essure is believed to be low risk and uneventful. But the allure of “non-incisional” permanent contraception as promised by HS would be substantially diminished if major surgery were required later [910]. Given the paucity of meaningful longitudinal data on HS patients, the hysterectomy rate following Essure remains undefined. Yet should this birth control choice even occasionally result in hysterectomy, caution is appropriate and the issue should receive close scrutiny. If the number of HS kits have been sold worldwide is 750,000 [22], then determining how these devices contribute to overall hysterectomy utilization represents a relevant topic in the domain of international women's health. Consideration should therefore be given to establishing an Essure patient registry, or, alternatively, creating specific ICD-10 codes for patients who present with HS-associated symptoms. These would be appropriate and cost-effective interventions to enable proper surveillance on this topic.



 XML Download
XML Download