

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Ectopic pregnancies account for 4% to 6% of all maternal death [1]. It has been known that medical treatment with methotrexate for unruptured tubal ectopic pregnancy is a safe and effective method [2]. Methotrexate traditionally is administered using a multi-dose regimen but single-dose regimen was developed for patient compliance and reduction of adverse effects [3].
An earlier meta-analysis reported that the use of single-dose regimen was associated with a significantly higher failure rate of methotrexate than the use of the multi-dose regimen (12% vs. 7%) [4]. A Cochrane review revealed that multi-dose regimen is comparable with laparoscopic salpingostomy, but a single-dose regimen is not effective compared to laparoscopic salpingostomy, as a result of inadequately declining serum human chorionic gonadotropin (hCG) concentrations after one single dose and necessitating additional methotrexate injections or surgical interventions [5]. According to those reports, multi-dose regimen appears to be more effective than single-dose regimen in treatment of tubal ectopic pregnancy.
However, subsequent two retrospective studies and two randomized trials reported a similar effectiveness between a single-dose and multi-dose treatment [6789]. Nonetheless, in those studies pretreatment serum hCG cutoff level to predict medical treatment success was not given in each regimen, thus it is still unknown which regimen is appropriate in a specific range of pretreatment serum hCG level.
High pretreatment serum hCG level has been known to be the most important predictor associated with medical treatment failure [241011121314]. In a review of 503 women with tubal pregnancy treated with a single-dose of methotrexate, failure rate in patients with serum hCG <5,000 IU/L was <4%, whilst the failure rate in patients with serum hCG 5,000 to 9,999 and ≥10,000 IU/L were 14% and 18%, respectively [10]. Therefore, pretreatment serum hCG level should be in consideration when comparing success rate between single-dose and multi-dose regimen.
If pretreatment serum hCG cutoffs to predict treatment success are different in both regimens, it would help us to decide which regimen be preferred in a specific range of initial serum hCG level. For example, a randomized trial reported a similar efficacy but different hCG cutoffs (3,600 and 5,500 IU/L) between single-dose and double-dose regimen [15]. This implies that single-dose regimen may be appropriate if initial serum hCG level is below 3,600 IU/L, but double-dose regimen is more favored if initial serum hCG level is between 3,600 and 5,500 IU/L. This strategy might maximize the overall medical treatment success of tubal ectopic pregnancy.
The aim of the present study was to investigate individual serum hCG cutoff to predict medical treatment success in single-dose and multi-dose regimen of methotrexate for tubal ectopic pregnancy.
Materials and methods
A single-institution retrospective study was conducted at the Seoul National University Bundang Hospital with the approval of the institutional review board (B-1601-332-101). In this study, 85 women who received methotrexate for the treatment of tubal ectopic pregnancy during 2003 to 2015 were selected. In the selection process, patients with a highly suspicious for tubal ectopic pregnancy by ultrasonograpy irrespective of pretreatment serum hCG titer were included. In addition, the patients with pregnancy of unknown location (PUL) that showed no visible gestational sac in intrauterine cavity, cervix, and ovary and with pretreatment serum hCG level ≥1,500 IU/L were also included. Patients with PUL with serum hCG level below 1,500 IU/L or unknown treatment result (e.g., loss of follow-up) after methotrexate treatment were excluded. The right tubal pregnancy was identified in 36 women and the left tubal pregnancy was identified in 31 patients; 18 women were assigned to be PUL. Fifty-three women received a single-dose regimen and 32 women received a multi-dose regimen. All patients were considered candidates for methotrexate therapy because their conditions were hemodynamically stable, did not have free peritoneal fluid in the pelvic cavity, and did not desire surgical treatment.
Age, parity, previous tubal ectopic pregnancy history, previous in vitro fertilization/intrauterine insemination, the week of gestation by last menstrual period, size and location of tubal ectopic mass, the presence of ectopic cardiac activity, and initial and following serum hCG level at day 4 to 7 were recorded. Size of tubal ectopic mass was defined as the maximum diameter in any dimension of the gestational mass as measured by ultrasound examination. If the gestational mass could not be differentiated from the tubal hematoma, the maximum diameter of the entire mass was used.
For single-dose regimen, intramuscular methotrexate 50 mg/m2 (body surface area) was administered. If subsequent serum hCG level failed to fall more than 15% of previous serum hCG between day 4 to 7 after methotrexate administration, a second dose was administered. Patients in the multi-dose regimen group received intramuscular methotrexate 1 mg/kg (body weight) was given on alternating days. Citrovorum as a rescue factor at dosage of 0.1 mg/kg was given on the each day after methotrexate injections. A second course of methotrexate/citrovorum was given if previously falling levels plateaued or rose on two consecutive serum hCG titers.
Failure with medical treatment defined as need for surgical intervention. Indications of surgery was classified as (1) insufficient fall or rise of serum hCG level, (2) rupture of tubal pregnancy, (3) clinical symptoms related to tubal pregnancy, or (4) sufficient fall of serum hCG level but presence of persistent mass.
All statistical analyses were performed by using the PASW ver. 18 (SPSS Inc., Chicago, IL, USA). When numeric data were compared between two groups, nonparametric Wilcoxon test was used and the data were expressed as median and 95% confidence interval for the median. The proportions were compared by using the chi-square test. If more than 25% of the expected cell values were less than 5, the Fisher exact test was applied instead. A receiver operating characteristics curve analysis was performed to estimate the pretreatment serum hCG titer to predict the success. Results were considered always significant when the P-value was <0.05.
Results
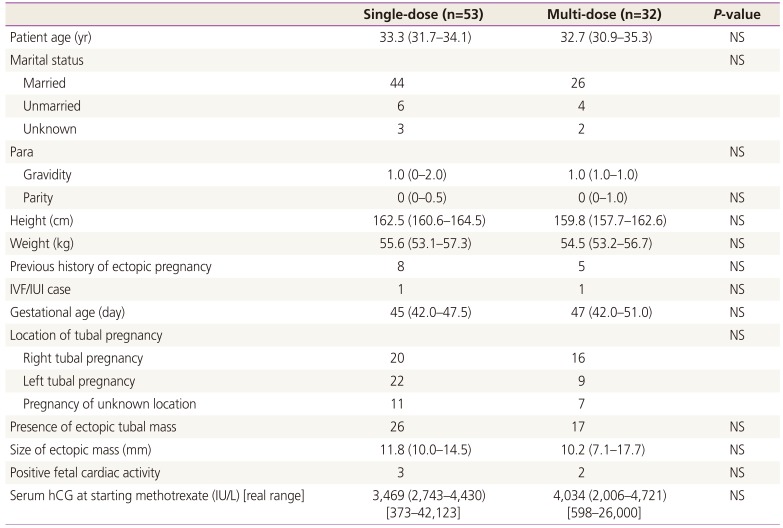
Before treatment, there were no statistically significant differences in the clinical and laboratory characteristics between the single-dose regimen group and multi-dose regimen group (Table 1). In the multi-dose regimen group, there was no case with additional cycle, but in 23 patients in the single-dose regimen group (43.4%), additional doses were administered. In detail, one additional dose was administered in 17 patients; additional doses were administered twice in 4 patients, and three times in 2 patients.
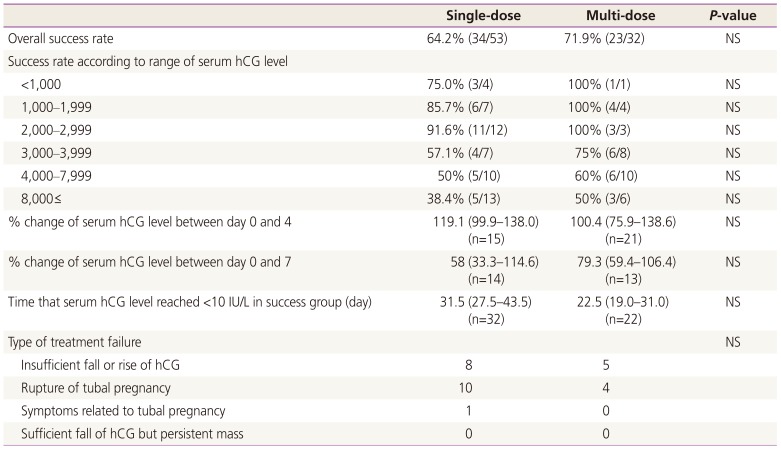
Overall treatment success rate was 67.1% and the success rate was not different between the single-dose and multi-dose regimen group (Table 2). When assessed according to the range of initial serum hCG level, success rate was generally good in cases with hCG level below 3,000 IU/L, but poor in cases with hCG level above 3,000 IU/L. The change of hCG level at day 4 and 7 over hCG level at day 0, time that hCG reached <10 IU/L in the success group, and type of treatment failure was similar between two regimen groups.
In the present study, maternal age, gestational age and size of ectopic mass were not predictor for treatment success and pretreatment serum hCG level was only prognostic factor for treatment success with a statistical significance (Table 3).
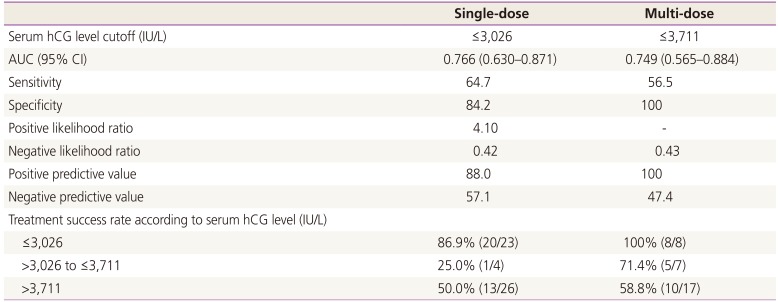
In the single-dose regimen group, serum hCG cutoff was 3,026 IU/L, whereas it was 3,711 IU/L in the multi-dose regimen group (Table 4). When serum hCG level was ≤3,026 IU/L, treatment success was generally good and similar in both regimens, however, when serum hCG level was between >3,026 IU/L and ≤3,711 IU/L, treatment success was better in the multi-dose regimen group, although statistically not significant. When serum hCG level was above 3,711 IU/L, treatment success was observed in approximately half of the patients in each regimen.
In the single-dose regimen group, initial serum hCG level (6,226 IU/L vs. 5,670 IU/L) and treatment success (60.0% vs. 69.6%) was similar between 30 patients without additional dose and 23 patients with at least one additional dose.
Discussion
In the present study, pretreatment serum hCG level was only prognostic factor for the prediction of treatment success, as like in other studies. Interestingly, serum hCG cutoff to predict the treatment success was different in two regimen groups; 3,026 IU/L in the single-dose regimen group and 3,711 IU/L in the multi-dose regimen group. Therefore, we proposed the choice of regimen according to different hCG interval; when serum hCG level was ≤3,026, single-dose regimen might be preferred because of its efficacy and convenience. However, when serum hCG level was between >3,026 IU/L and ≤3,711 IU/L, multi-dose regimen might be preferred because it is more efficacious than single-dose regimen. When serum hCG level was above 3,711 IU/L, both regimen could be used as clinician's preference but we emphasized that high risk of surgical intervention should be considered.
In previous four studies, similar effectiveness between a single- and multi-dose regimen have also been reported, but slightly higher treatment success was noted in the multi-dose regimen group in all studies [6789]. When the data from previous four studies and our study were pooled, the treatment success was similar between both regimens (87.1% vs. 89.9%). It is important to note that we did not consider cases with additional doses in the single-dose regimen group as treatment failure. If such cases were classified into the treatment failure in our data, success rate might be profoundly lowered (64.2% to 34%). Overall treatment success rate was low in the present study and one of the reasons for this observation might be inclusion of patients with a relatively high hCG titer (over 5,000 IU/L). In general, cases with serum hCG >5,000 IU/L are considered as relative contraindication of medical treatment [16]. Other reason might be exclusion of patients with PUL with serum hCG <1,500 IU/L.
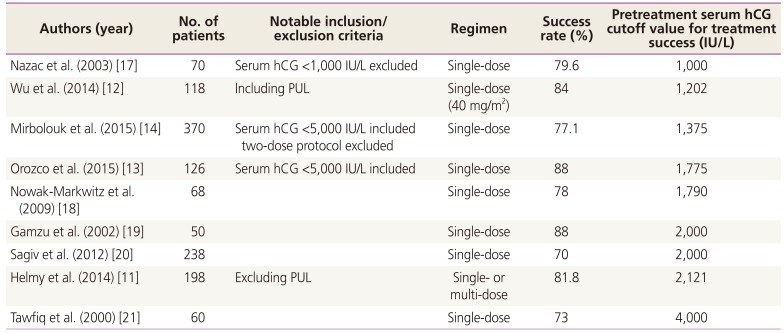
In the literature, various serum hCG cutoff values have been reported, mostly from single-dose regimen (Table 5) [111213141718192021]. In most of studies, inclusion criteria set by pretreatment serum hCG level or characteristics of enrolled patients were quite different, thus caution is needed for its interpretation. For example, only patients with hCG levels under 5,000 IU/L were included in two studies [1314]. In the study by Wu et al. [12], relatively lower cutoff value was suggested possibly because they included PUL. In contrast, relatively higher cutoff value was suggested in the study by Helmy et al. [22] possibly because they excluded PUL. In our study, relatively higher cutoff value was obtained possibly because we excluded PUL with serum hCG level <1,500 IU/L.
It has been known that approximately 15% to 20% of patients in the single-dose regimen require a second dose of methotrexate due to suboptimal decrease of serum hCG level between day 4 and 7 [41123]. In the present study, high portion of the patients (43.4%) who received single-dose regimen required additional doses. Because many patients need additional doses, double-dose regimen was developed. Barnhart et al. first described double-dose protocol that balances efficacy and safety on the one hand and convenience on the other hand [23]. Subsequently, a randomized trial reported a similar efficacy between single-dose and double-dose regimen [15]. In sub-group analysis in the present study, similar treatment success was also observed between group with and without additional dose. Therefore it is questionable whether double-dose regimen is superior to single-dose regimen.
In one retrospective study, a high failure rate (53%) of medical treatment has been reported in those with tubal pregnancy with serum hCG level >10,000 IU/L [24]. In that study, treatment failure rate was 62.5% in single-dose regimen and 33.3% in double- or multi-dose regimen. In our study, when including patients with serum hCG level >10,000 IU/L only, treatment failure rate was 77.7% (7/9) in single-dose regimen and 66.6% (2/3) in multi-dose regimen (overall failure rate 75%). Therefore, operation should be considered as the first-choice of treatment when serum hCG level is over 10,000 IU/L. Nonetheless, the highest serum hCG level at which methotrexate can be safely administered without increasing the risk of ectopic rupture has not been established. Among treatment success group in the present study, the highest serum hCG level was 26,000 IU/L in the multi-dose regimen and 15,079 IU/L in single-dose regimen.
Treatment of ectopic pregnancy can be surgical or medical. Nowadays, laparoscopic surgical and medical treatment with methotrexate is commonly used. American College of Obstetricians and Gynecologists (ACOG) suggested that medical management with methotrexate is safe and effective in properly selected population [25]. According to ACOG guidelines, the properly selected population include those patients with hemodynamically stable and no evidence of rupture. ACOG guidelines also suggested relative contraindications for medical therapy, which include gestational sac larger than 3.5 cm and embryonic cardiac motion because success rates are low in the population. An ectopic mass size less than 3 to 4 cm is also commonly used as a patient selection criterion; however, this has not been confirmed as a predictor of successful treatment [2]. A tendency towards a lower size of ectopic mass was observed in the successful methotrexate therapy group, but not significant [22]. We also found that size of ectopic mass was not predictor for treatment success.
The weakness of this study is enrollment of relatively small number of patients. Possible explanation for this might be exclusion of PUL with pretreatment serum hCG level <1,500 IU/L. However, our study presented pretreatment serum hCG cutoff values for each regimen and this might be helpful to decide effective regimen for medical treatment of tubal ectopic pregnancy according to specific range of hCG titer. Further large-scaled prospective study will be needed to confirm our conclusion.

 XML Download
XML Download