

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Cervical infection with human papillomavirus (HPV) is the main risk factor for the development of cervical intraepithelial lesions and cancer. Although most HPV infections disappear within one year, persistent infection in women can develop into cervical cancer. Furthermore, infection with specific high-risk HPV types has been associated with HPV persistence and progression to cervical cancer [12]. Therefore, HPV typing is clinically valuable and important for evaluating the possibility of cervical carcinogenesis [34].
In addition, several studies have reported that progression to cervical cancer is associated with various other factors, including HPV viral load [567], HPV integration [89], coinfection with multiple HPV types [1011], and epigenetic modifications of HPV DNA and host DNA [1213]. High viral load, in particular, is associated with not only HPV persistence, but also high-grade, progressive cervical lesions [1415]. Evaluation of both viral load and HPV type in cervical cancer screening is thought to be helpful for prediction of HPV persistence and cervical carcinogenesis, and for proper management of women who have HPV infections. Furthermore, evaluation of HPV type is important for monitoring the impact of the vaccines that protect against a limited number of genotypes [161718]. For therapeutic vaccines under development, HPV typing will be important to determine the elimination of a specific virus type [19].
In this study, we have described a new HPV diagnostic assay, the Cheil HPV DNA Chip, which makes it possible to quantify and identify HPV types at the same time using quantitative real-time (qRT) polymerase chain reaction (PCR) and microarray analyses. Moreover, we compared the accuracy of the Cheil HPV DNA Chip with that of conventional diagnostic kits.
Materials and methods
1. Study population
Among the women who visited the gynecologic oncology center at Cheil General Hospital and Women’s Healthcare Center between November 2009 and October 2011, 470 Korean women consented to participate in this study. This research was approved by the institution’s ethics committee (institutional review board no. CGH-IRB-2009-56). The mean age of the participants was 39.1 years (standard deviation [SD], 9.6], with a range of 17 to 77 years.
For HPV tests and Papanicolaou smear, cervical swabs were obtained from all 470 participants. The first cervical swab was obtained using Rovers Cervex-Brush and SurePath preservative fluid (BD TriPath, Burlington, NC, USA) for the Papanicolaou smear, HPV DNA chip tests, and HPV sequencing analysis. The second swab was obtained using the DNAPap Cervical Sampler (Qiagen, Gaithersburg, MD, USA) to perform the Hybrid Capture II test (HC II). Cervical cytology of all participants was classified as normal (n=30), atypical squamous cells of undetermined significance (ASC-US, n=192), atypical squamous cells-cannot exclude high-grade squamous intraepithelial lesion (ASC-H, n=47), low-grade squamous intraepithelial lesion (LSIL, n=93), high-grade squamous intraepithelial lesion (HSIL, n=93), and cancer (n=15).
2. Isolation of DNA
Five milliliter of the liquid-based cervical sample was used for cervical cytology. The other 5 mL of the liquid-based cervical specimen was stored at 4℃ before isolation of DNA. DNA was isolated using a DNeasy Blood and Tissue Kit (Qiagen, Valencia, CA, USA), according to the manufacturer’s instructions, in 100 µL of elution buffer (Qiagen) and was stored at -20℃.
3. Cheil HPV DNA Chip assay
The Cheil HPV DNA Chip method for quantification and genotyping of HPV was based on SYBR Green I qRT-PCR and a microarray assay. In the qRT-PCR step, we prepared genomic DNA from clinical samples and serially diluted positive controls at concentrations ranging from 1×106 to 1×102 copies to generate a standard curve (y=-3.507x+40.87, r2=0.99) (Supplemental Fig. 1). All templates were amplified with GPM7 F, GPM7 F2, and GPM7 R primers for quantification of HPV copy numbers. In addition, qRT-PCR for human beta globin was performed with HBB-F/R primers for normalization of HPV copy numbers in each sample. Melting temperature values were used to discriminate primer dimers (formed at a melting temperature of approximately 70℃) from target PCR products that appear at an approximate melting temperature of 78℃ to 86℃. In the microarray assay step, we used products generated from the qRT-PCR step directly for genotyping on a DNA chip slide, the Cheil HPV DNA Chip, that was spotted with sequence specific probes for high-risk HPV, low-risk HPV, and human beta globin as a control.
In more detail, novel consensus primers (GPM7 F, GPM7 F2, and GPM7 R) were designed for the broad detection of HPV types. The nucleotide sequences (5’-3’) of GPM7 F, GPM7 F2, and GPM7 R were AGTGGTCATCCWTTWTTWAATAAATTKGATGA, AGTGGCCATCCWTTDTWKAATAGGYWKGATGA, and Cy5-CCAWAGCCWGTATCWACCATRTCACCATC, respectively (W: A or T; K: G or T; D: A, G or T; Y: C or T; R: A or G). These primers targeted the conserved L1 region located upstream of MY09/11. Two forward primers were adopted to overcome the HPV type-dependent PCR efficiency, and Cy5 was used as a label for the reverse primer for identification of HPV types on the Cheil HPV DNA Chip.
The SYBR Green qRT-PCR reaction for detection and quantification of HPV was performed with 4 pmol of forward primers, 8 pmol of Cy5-labeled reverse primer, 10 µL of 2× SYBR Green I Master Mix (Roche Diagnostics, Mannheim, Germany), 0.5 units of uracil DNA glycosylase (UDG; New England Biolabs, Ipswich, MA, USA) to prevent cross contamination, and 2 µL of sample DNA or positive control. A SYBR Green qRT-PCR reaction for human beta globin was used as an internal control, and the normalization factor was almost identical to that of HPV. The nucleotide sequences (5’-3’) of the HBB-F/R primer set for amplifying human beta globin were TCTGTCCACTCCTGATGCTG and Cy5-TCAAGCGTCCCATAGACTCA, respectively. SYBR Green qRT-PCR was performed at 37℃ for 10 minutes for the UDG reaction, which was followed by incubation at 95℃ for 10 minutes and followed by 45 cycles of 95℃ for 10 seconds, 55℃ for 10 seconds, and 72℃ for 10 seconds. Fluorescence was detected during the extension time and melting analysis was performed at temperatures between 65℃ and 95℃.
Each product from the SYBR Green qRT-PCR of HPV and human beta globin (5 µL) was denatured in a tube at 95℃ for 10 minutes and immediately transferred to an ice-ethanol bath. The mixture containing qRT-PCR products and hybridization buffer (5× saline-sodium citrate [SSC], 0.2% sodium dodecyl sulfate) was slowly injected into the hole of the cover slip on the Cheil HPV DNA Chip. The hybridization was performed at 60℃ for 20 minutes under high humidity. After hybridization, the slides were washed with washing solution (1× SSC, 0.1% sodium dodecyl sulfate) three times and rinsed with 1× SSC three times.
After the slides were dried, HPV types were identified using a chip scanner (NimbleGene MS 200, Tecan, Salzburg, Austria) and analyzed with GenePix Pro 6.0 software (Axon Instruments, Union, CA, USA). The samples were analyzed for the presence of high-risk HPV types (16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 67, 68a, 68b, 69, and 82) and low-risk HPV types (6, 11, 30, 32, 40, 42, 43, 44, 54, 55, 62, 70, 72, 81, 84, 90, and 91).
All the materials and procedures used for this kit were approved by the Ministry of Food and Drug Safety in Korea (no.14-2715).
4. Conventional HPV DNA Chip assay
A conventional HPV DNA chip method was performed with the GG HPV DNA Genotyping Chip Kit (Goodgene, Seoul, Korea) according to the manufacturer’s protocol. After the PCR reaction using 5 µL of DNA sample, 10 µL of HPV product and 5 µL of human beta globin product were denatured in tubes at 95℃ for 3 minutes and immediately transferred to ice. A mixture containing PCR products and 65 µL of hybridization buffer was injected onto the HPV DNA chip and allowed to hybridize with probes at 48℃ for 30 minutes. After hybridization, DNA chip slides were washed with washing buffers I and II, and dried with a spin dryer. The HPV DNA chip was visualized a chip scanner and analyzed using GenePix Pro 6.0 software. The samples were analyzed for the presence of high-risk HPV types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68, and 69) and low-risk HPV types (6, 11, 34, 40, 42, 43, and 44).
All the materials and procedures used for this kit were approved by the Ministry of Food and Drug Safety in Korea.
5. HC II assay
HPV DNA titer was measured with the HC II High-Risk HPV DNA Test Kit (Qiagen, Gaithersburg, MD, USA) according to the manufacturer’s protocol. The cutoff value (CO) was 1 pg/mL, which is equivalent to 5,000 copies of HPV type 16 per assay. Samples were classified as HPV DNA-positive if the relative light unit (RLU) reading obtained from the luminometer was equal to or greater than the mean value of the positive controls provided by the manufacturer. The samples were analyzed for the presence of high-risk HPV types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68).
6. HPV type-specific PCR and sequencing analysis
HPV type-specific PCR was performed with type-specific primers that were selected based on results from both the Cheil HPV DNA Chip and the GG HPV DNA Genotyping Chip Kit for all samples. For example, when HPV 16 was detected by both kits, HPV 16-specific primers were used for PCR. If HPV 16 was detected by one kit and HPV 18 was detected by the other kit, HPV 16- and HPV 18-specific primers were both used for HPV type-specific PCR. Type specific primers are targeted to the L1 regions of high-risk HPV types (16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 67, 68a, 68b, 69, and 82) and low-risk HPV types (6, 11, 30, 32, 40, 42, 43, 44, 54, 55, 62, 70, 72, 81, 84, 90, and 91) (Supplemental Table 1).
The purified PCR products were subjected to sequencing using the ABI PRISM BigDye Terminator Cycle Sequencing Kit (Applied Biosystems, Foster City, CA, USA) to confirm the HPV genotype. The sequencing analyses were performed using an ABI PRISM 3100 Genetic Analyzer (Applied Biosystems).
7. Construction of a positive control plasmid
Coding sequences for the L1 region of HPV16 (1,401 bp) derived from CaSki cells and human beta globin (193 bp) were inserted into the same vector (pGEM T Easy Vector, Promega, Madison, WI, USA). Serially diluted positive controls at concentrations of 5×105, 5×104, 5×103, 5×102, and 5×101 copies/µL were used to generate a standard curve for qRT-PCR.
8. Statistical analyses
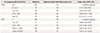
Cohen’s kappa values with 95% confidence intervals (CIs) were calculated to evaluate the agreement between the results of sequencing and the HPV DNA Chip assays or HC II. As HC II does not provide typing results, and the detectable HPV types differed among the samples tested, the assays were compared at the level of each detectable HPV type, with positive versus negative detection evaluated according to the sample (Table 1). The two-sided McNemar chisquare test was used to determine the correlation between high-risk HPV and disease severity (Table 2). P-values from Kruskal-Wallis test with Scheffe using ranks were used as a post hoc study for viral load and RLU/CO among the different cytological categories (Fig. 1). Odds ratios (ORs) with 95% CI were used to assess the risk of abnormal cytology, especially for LSIL/HSIL/cancer, at a given viral load and RLU/CO (Table 3).
Results
1. Comparative analyses of the Cheil HPV DNA Chip and conventional HPV diagnostic tests
We compared the Cheil HPV DNA Chip with the GG HPV DNA Genotyping Chip using 470 genital samples. HPV type-specific PCR and sequencing analysis was used as a reference test to compare the assays by kappa statistical analysis.
Kappa values less than 0.2 or over 0.81 represented “slight” or “almost perfect” agreement, respectively. In addition, values of 0.21 to 0.4, 0.41 to 0.6, and 0.61 to 0.8 represented “fair”, “moderate”, and “substantial” agreement, respectively [20]. The agreement between the reference test and the Cheil HPV DNA Chip method was 98.5% (k=0.963; 95% CI, 0.919 to 0.98), whereas 77.9% (k=0.527; 95% CI, 0.447 to 0.59) agreement was shown between the reference test and the GG HPV DNA Chip method (Table 1).
2. Qualitative analysis with the Cheil HPV DNA Chip
We performed a qualitative analysis of HPV DNA genotypes using the Cheil HPV DNA Chip on 470 genital samples and found 339 (72.13%) women with HPV infection and 131 (27.87%) women without infection. HPV DNA genotyping identified 63 (13.40%) women with HPV 16, 26 (5.53%) with HPV 52, 22 (4.68%) with HPV 58, 16 (3.4%) with HPV 51, and 16 (3.4%) with HPV 56. Multiple types of HPV infection were detected in 44 (10.0%) women (Table 2). There was a higher occurrence of high-risk HPV types in cervical samples with greater disease severity (chi-square=23.396, P<0.01). High-risk HPV was detected more frequently in samples with high-grade lesions than in those with low-grade lesions: 30% in normal, 38.1% in ASC-US/ASC-H, 53.8% in LSIL, 77.4% in HSIL, and 100% in cancer.
Furthermore, the results for HPV 16 (chi-square=62.28, P<0.01), HPV 33 (chi-square=7.18, P<0.01), and HPV 58 (chi-square=9.52, P<0.01) were significantly different with respect to disease severity.
3. Quantitative analysis by cytologic categories
We quantified HPV copies in all 470 samples by SYBR Green qRT-PCR and normalized the number of viral copies per cervical cell. Viral loads determined by the Cheil HPV DNA Chip show significant differences among the overall cytological categories (P<0.001, by Kruskal-Wallis test). The average viral load was 1.49 (SD, 4.86) in normal, 8.47 (SD, 43.47) in ASC-US/ASC-H, 83.65 (SD, 276.14) in LSIL, 97.04 (SD, 393.61) in HSIL, and 91.30 (SD, 179.26) in cancer (Fig. 1A). The RLU/CO determined by HC II also showed an increasing trend with the cytological categories (P<0.001, by Kruskal-Wallis test). The average viral load was 90.38 (SD, 252.46) in normal, 127.02 (SD, 353.36) in ASC-US/ASC-H, 475.34 (SD, 984.23) in LSIL, 402.82 (SD, 702.54) in HSIL, and 520.54 (SD, 686.98) in cancer (Fig. 1B). For further analysis, a significant mean difference was shown between ASC-US/ASC-H and LSIL in both viral load (P<0.001) and RLU/CO (P<0.001). This suggests that the viral load and RLU/CO have a trend of increasing in range from ASC-US/ASC-H to LSIL. However, there were no statistically significant differences between LSIL, HSIL, and cancer (P>0.05 in post hoc test).
To evaluate the possible relationship between viral load and the cytological categories, ORs were calculated for five groups of viral loads (0 to <0.1, 0.1 to <1, 1 to <10, 10 to <100, and ≥100) and RLU/CO values (0 to <1, 1 to <10, 10 to <100, 100 to <1,000, and ≥1,000). There was a significant association between LSIL/HSIL/cancer and viral loads above 0.1 copies/cell (OR, 2.75; 95% CI, 1.64 to 4.64) and RLU/CO above 1.0 pg/mL. The OR was greatest in infections with viral loads above 100 copies/cell (OR, 12.21; 95% CI, 4.77 to 31.25).
Discussion
Various methods have been used for HPV detection. Among these, the HC II assay is a convenient, semi-quantitative signal amplification method. However, the HC II system has limitations in analyzing HPV genotype because it employs heterogeneous probes in a single reaction that does not distinguish between the genotypes hybridized. Target amplification methods such as PCR are flexible and sensitive, and qRT-PCR is an advanced technique that allows quantification of the copy number of the gene of interest. DNA microarrays are most often applied to gene expression profiling and mutational analyses. Because a microarray can include many probes with various sequences, microarray analysis can accomplish multiple genetic tests in parallel. Therefore, microarrays are suitable for identifying the HPV type from among the approximately 100 distinguishing genetic variations.
In this study, we adopted two key advantages from the various available methods: the ability to quantify viral load by qRT-PCR and the capacity for high-throughput screening of genotypes by the Cheil HPV DNA Chip microarray. Although the commonly used consensus primers, MY09/10, GP5+/GP6+, PGMY, and SPF10, target highly conserved regions of HPV L1 and are thus used for the detection of a broad range of HPV types, some studies have shown that sensitivity of PCR with these primers varies with HPV type [2122]. In addition, these consensus primers can give discordant results when applied to coinfected samples [2122] because they do not precisely match the target sequence for all HPV types. A similar problem occurred when we adopted GPM7 F as our only forward primer in the SYBR Green qRT-PCR. Specifically, this primer was not sufficiently sensitive for the detection of HPV types 39, 40, 68, and 84. To achieve greater efficiency in the detection of all types of HPV, we determined that two forward primers, GPM7 F and GPM7 F2 (data not shown). It is believed that equivalent PCR efficiency is important for obtaining reproducible results in the qRT-PCR and genotyping stages. Therefore, our method can be expected to be more reliable than other methods. As shown in the comparison analysis in Table 1, the kappa values (k=0.963; 95% CI, 0.919 to 0.98) demonstrate that our method was superior to the GG HPV DNA Chip (k=0.527; 95% CI, 0.447 to 0.59).
In the HPV DNA genotyping of clinical samples using the Cheil HPV DNA Chip (Table 2), HPV 16 was the most prevalent type, and HPV 52 and 58 also showed a high frequency in this study. HPV 16 is the most reliable predictor of persistent HPV infection [1], and HPV 52 and HPV 58 are dominant genotypes in Korean women [23]. This study shows the overall prevalence of HPV was 72.13%. This rate is higher than that found by other studies [242526], because participants of this study were referred to the gynecologic oncology center from local clinics due to abnormal cytology or HPV infection. In addition, high-risk HPV types, 16, 33 and 58, were detected at significant levels among samples from high-grade disease lesions.
Our study also assessed high viral loads as a risk factor for abnormal cytology. ORs for LSIL/HSIL/cancer were higher with high viral loads (Table 3). This is consistent with the results in Fig. 1 that shows that higher-grade lesion groups have higher viral loads. However, the CIs tended to be broad for the viral load, suggesting that more samples need to be analyzed to verify the tendency of increasing ORs.
Although the small sample size in this study was a limitation, we could validate this method by determining correlations among HPV type, viral load, and disease severity in cytological categories.
In conclusion, the Cheil HPV DNA Chip is an effective diagnostic method to simultaneously detect HPV genotype and viral load in cervical samples. Our future research will clarify the relationship between viral loads of specific HPV genotypes and progression of cervical intraepithelial lesions.



 XML Download
XML Download