

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Tamoxifen has been widely used for adjuvant treatment of breast cancer, but several gynecological side effects after its use have been noted, including endometrial hyperplasia, endometrial polyps, endometrial carcinoma, and rare complications such as endometriosis, adenomyosis, and cervical polyps [123]. Polypoid endometriosis is a rare benign gynecological disease, and several reported cases were associated with the use of tamoxifen [2]. To the best of our knowledge, three cases of polypoid endometriosis have been reported in the Korean literature, but in none of the cases, polypoid endometriosis was associated tamoxifen use. Herein, we report the first case of polypoid endometriosis associated with tamoxifen treatment in a breast cancer patient.
Case report
A 66-year-old woman, who had received left partial mastectomy due to ductal carcinoma in situ about 4 years ago and was taking tamoxifen treatment until a recent date, was admitted for evaluation of an incidentally detected ovarian cyst. She had reached menopause 10 years ago and had no other medical history except that she was a carrier of hepatitis C virus. In the laboratory findings, liver enzymes showed an occasional increase but there was no specific problem, and CA-15-3 was within the normal range. Although the initial pelvic sonography in breast cancer work-up showed no abnormal findings, the second pelvic sonography performed 2 months before hysterectomy revealed thickened endometrium (9.7 mm), suggesting endometrial hyperplasia, and a right ovarian cyst (41×36×35 mm). Pelvic magnetic resonance imaging revealed multiple cystic structures in the endometrial cavity with mildly thickened endometrium and an approximately 4.1×3.4-cm-sized, well-defined, multicystic lesion in the right ovary with peripheral enhancement, suggestive of tamoxifen-associated endometrial and ovarian changes (Fig. 1). Under the impression of endometrial hyperplasia and right ovarian cyst, she received hysterectomy with bilateral salpingooophorectomy. The right ovarian mass, which was detected by radiologic examination, was confirmed to be a right paratubal mass.
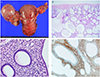
Grossly, a 4×3-cm-sized, well-circumscribed, polypoid mass was noted in the right paratubal area (Fig. 2A). Microscopically, it revealed a multilocular cystic structure comprising of cystically dilated endometrial glands and stroma together (Fig. 2B). No hyperplastic feature or complexity of glands was noted. There were no areas of fibrosis, necrosis, and decidual change in the stroma. The glands were lined by a single layer of columnar or cuboidal cells with no identifiable cellular atypia or mitosis (Fig. 2C). Both glandular epithelial cells and stromal cells were positive for estrogen receptor (not shown in figure). Presence of CD10-positive stromal cells confirmed the endometrial nature (Fig. 2D). She was diagnosed as having an endometrial polyp with cervical endometriosis and paratubal polypoid endometriosis and was discharged without any complications.
Discussion
Endometriosis is an estrogen-dependent disorder, and it is rare in postmenopausal women. There are a growing number of cases in the literature, which suggest that the tamoxifen is an antagonist of the estrogen receptor in breast tissue but behaves as an agonist in the endometrium, and is associated with the development of endometriosis in post-menopausal woman with breast cancer [345].
Since Mostoufizadeh and Scully [6] first described polypoid endometriosis in 1980, it has been considered as a benign gynecologic lesion that develops in endometriosis. It usually simulates a malignant tumor during the operation and histologically resembles an endometrial polyp. According to the review of 24 cases of polypoid endometriosis by Parker et al. [7], polypoid endometriosis showed several clinico-pathologic differences when compared with typical endometriosis. It usually occurred in an older age group; 60% of patients with polypoid endometriosis in their study were more than 50 years of age as compared to <5% of patients with typical endometriosis. The authors also mentioned that hormonal factors might play a role in its pathogenesis, including its association with tamoxifen treatment.
Pathologically, polypoid endometriosis should be differentiated from other neoplasms, such as adenofibroma and adenosarcoma due to the presence of benign glands. Indeed, focal or diffuse architectural atypia of the glandular epithelium can be observed in the above lesions. However, endometrioid adenofibroma usually has an ovarian-type stroma in contrast to the endometrial-type stroma of polypoid endometriosis. Adenosarcoma can be distinguished from polypoid endometriosis because the former has projecting stromal papillae or broad polypoid fronds, atypia of stromal cells, and periglandular cellular stromal cuffs.
In conclusion, three cases of polypoid endometriosis have been reported in Korea; in two cases, polypoid endometriosis originated from the rectum mimicking rectal cancer, and in one case, it developed as a subserosal mass in the uterus [8910]. However, in none of the cases, polypoid endometriosis was associated with tamoxifen use, and this is the first report of tamoxifen treatment-associated with polypoid endometriosis in Korea.

 XML Download
XML Download