

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Spontaneous abortion (SA) is defined as the loss of fetal product before 20 weeks of gestation [1]. Ten percent to 15% of clinically recognized pregnancies end in SA and the total pregnancy loss is estimated to be 30% to 50% of all conceptions [2,3,4]. The most frequent cause of SA is fetal chromosome abnormalities. The frequency of chromosome imbalance in SA is at least 50% in the first trimester and 20% in the second [5].
Recurrent miscarriage (RM) is defined as the occurrence of three or more consecutive losses of pregnancy. According to this definition, it affects about 1% of couples trying to have a baby [6]. However, many clinicians define RM as two or more losses; this increases the percentage of RM from 1% to 5% of all couples trying to conceive [7]. Chromosome abnormalities, like SA, are the most common cause of RM. About 50% to 60% of all miscarriages are associated with cytogenetic abnormalities, the most frequent being trisomy, followed by polyploidy and monosomy X [6,8,9,10].
RM is a very frustrating condition for both the couple and the clinician, because it is difficult to find a distinct reason for the repeated failure to sustain a pregnancy and eventually have a successful pregnancy outcome. Epidemiologically, advanced maternal age is a strong risk factor for both SA and RM. The number of good quality oocytes in older mothers is fewer than younger mothers, which increase the frequency of chromosomal abnormalities leading to miscarriage [11,12,13]. The risk of further miscarriage increases to approximately 50% for women with three or more losses without a liveborn infant [14,15].
Karyotyping of miscarriage tissues in couples with SA or RM is not routine practice. More data on the karyotype of miscarried conceptuses need to be collected, which may be helpful for both the patients and the physicians. However, there are few studies comparing the frequency of chromosome abnormalities in miscarriages from couples with and without RM. One of these studies consists of 420 miscarriages from 285 couples with RM. In this report, 54% of the miscarriages were euploid and 46% were cytogenetically abnormal [8].
The primary objective of this study was to determine the frequency and distribution of cytogenetically abnormal miscarriages from couples with SA or RM and to see whether or not there was any difference in the frequency and distribution of chromosome abnormalities between the first pregnancy loss (SA) and two or more losses (RM). Our hypothesis was that if the non-cytogenetic factors were excluded, the rate of cytogenetic abnormality in RM group might be higher compared with SA group and that the frequency of euploid miscarriages would be decreased compared with the previous reports.
Materials and methods
1. Patients
A retrospective cohort analysis was conducted with patients referred to the Genetics Laboratory of Good Moonhwa Hospital from 2000 to 2013. All the enrolled cases have no identified causes for abortions and the following cases were excluded: A case of twin pregnancy, 2 cases in which cell culture was failed, 3 cases derived from parental chromosomal abnormality (a case of Robertsonian translocation and 2 cases of balanced translocation), 19 cases of spontaneous pregnancy losses in which the gestational ages are >21 week and cases with non-cytogenetic factors (antiphospholipid syndrome, uterine abnormalities, endocrine abnormalities, immune dysfunction, etc.).
The patient population consisted of 250 Korean women referred for evaluation of fetal death and having at least one or more pregnancy losses. They were divided into two groups: SA or RM group. SA group consisted of 164 cases from couples with the first pregnancy loss. 86 cases offered from couples with two or more pregnancy losses were considered as RM group. The fetal demise was diagnosed by ultrasound scan and the gestational age of abortuses was estimated by dating the last menstrual period at the time of diagnosis.
This study was approved by local ethics committee of Good Moonhwa Hospital. Written informed consent was obtained from all study subjects prior to enrollment in the study. Local Institutional Review Board approval was obtained to extract data from patient's medical records.
2. Tissue treatment
The abortus tissues were minced into very small fragments and trypsinized with 0.25% trypsin for 30 minutes. After then, samples were centrifuged at 1,500 rpm for 5 minutes and the supernatant was removed. The pellet was resuspended in Chang media containing 1 mg/mL collagenase I and incubated for 1 hour at 37℃ in shaking incubator. The preparation was then centrifuged at 1,500 rpm for 5 minutes, the supernatant was aspirated, and the cell pellet was washed and resuspended in Chang media. Cells were then cultured until they were nearly confluent. At that time of confluency, cells were harvested and slides for karyotyping were prepared.
3. Cytogenetic analysis
Cytogenetic results of the enrolled 250 cases were all successfully analyzed. Karyotyping was performed by GTG banding technique at approximately 400 to 550 band level. Twenty metaphases were analyzed in all cases except for mosaicism, which was analyzed up to 50 metaphases. The chromosomal status was analyzed using CytoVision from Applied Imaging (New Castle, UK). Chromosomal abnormalities were reported according to An International System for Human Cytogenetic Nomenclature (ISCN 2009).
Results
The patient age of SA group ranged from 19 to 42 years, with a mean of 30.3 years and that of RM group ranged from 25 to 41 years, with a mean of 31.9 years. In Tables 1 and 3, in addition to the category of maternal or estimated gestational age, cytogenetic results were shown as number of normal (euploidy) and abnormal chromosomes. In Tables 2 and 4, abnormal chromosomes were further subdivided into trisomy, monosomy X, polyploidy, and structural aberrations.
Among the total 164 cases of SA group, 81 cases (49.4%) were euploid and the rest (83 cases, 50.6%) showed chromosomal abnormalities. In RM group with two or more pregnancy losses (RM[≥2]), 31 (36.0%) cases were euploid and 55 (64.0%) cases were abnormal. In RM group with three or more pregnancy losses (RM[≥3]) (8 cases with the 2nd pregnancy loss were excluded), 27 (34.6%) cases were euploid and 51 (65.4%) cases were abnormal. The frequency of abnormal cases in both RM group was higher than that in SA group and showed a statistically significant difference (P<0.05) (Tables 1, 3).
Abnormal chromosomes analyzed in this study included trisomies, monosomy X, polyploidy, mosaicisms, and structural aberrations. Among the total 83 abnormal cases in SA group, 53 (63.9%) were trisomic (including double or triple trisomies), 12 (14.5%) were monosomic X, 6 (7.2%) were polyploid, 6 (7.2%) were mosaicisms or marker chromosomes and 6 (7.2%) were structural aberrations (including deletions, isochromosomes and unbalanced translocations). In RM(≥2) and RM(≥3) group, 45 (81.8%)/42 (82.3%) were trisomic (including double or triple trisomies), 2 (3.6%)/1 (2.0%) were monosomic X, 5 (9.1%)/5 (9.8%) were polyploid and 3 (5.5%)/3 (5.9%) were structural aberrations (including deletions, isochromosomes and unbalanced translocations), respectively. There was a significant difference in the distribution of trisomic and monosomy X cases between SA and RM group (P<0.05) (Tables 2, 4).
The distribution of cytogenetic diagnosis of SA or RM group, stratified for the maternal age, was analyzed in Tables 1 and 2. Patients were subdivided by maternal age into the following groups: <30 years, 30 to 34 years and ≥35 years. In both groups, women with advanced maternal age (≥35 years) had a higher rate of chromosome anomalies compared with women younger than age 35 (normal:abnormal = 32.4%:67.6% for ≥35 years and 53.8%:46.2% for <35 years in SA; 19.2%:80.8% for ≥35 years and 43.3%:56.7% for <35 years in RM[≥2]; 21.7%:78.3% for ≥35 years and 40.0%:60.0% for <35 years in RM[≥3]; P<0.05).
The distribution of cytogenetic diagnosis of SA or RM group, stratified for the estimated gestational age, was analyzed in Tables 3 and 4. Patients were subdivided by the estimated gestational age into four groups: <10 week, 10 to 15 week, and 16 to 20 week. Among 164 cases of SA group, 71 were in <10 week, 58 in 10 to 15 week, and 35 in 16 to 20 week. An increase of normal (euploidy) karyotypes was noted with increased gestational age (<10 week, 38.0%; 10-15 week, 53.5%; 16-20 week, 65.7%). In contrast to the results of SA group, RM group showed most of cases (77/86 and 70/78) were in <10 week (Table 3). In all groups, the most common chromosome abnormality in miscarriages before 10 weeks of gestation is autosomal trisomy, followed by ployploidy such as triploidy or tetraploidy and monosomy X (Table 4).
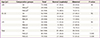
The distribution of cytogenetic diagnosis in SA or RM(≥2) group with aneuploidy according to the estimated gestational age was further analyzed in Tables 5 and 6. In both groups, the most frequent trisomic was 16 (11 cases for SA, 10 cases for RM[≥2]), followed by trisomies 22 (9 cases for SA, 10 cases for RM[≥2]) and 21 (7 cases for SA, 4 cases for RM[≥2]). Notably, abortions with trisomies of lower number chromosomes (chromosomes 1-12) were mostly occurred in <10 week except for two cases (one with trisomy 12 for 10-15 week in SA, one with trisomy 9 for 16-20 week in RM[≥2]) and the frequency of abortions with trisomies of these lower number chromosomes was increased in RM(≥2) compared with that of SA. In addition, most of aneuploidies in RM(≥2) (94.2%) were occurred at the estimated gestational age of <10 week and this frequency was considerably different from that of SA (55.8%).
Discussion
Cytogenetic studies give the important genetic information and thus act as a good genetic tool. This study has focused on determining the frequency and distribution of cytogenetically abnormal miscarriages from couples with SA or RM and analyzing any difference in the frequency and distribution of chromosome abnormalities between the first pregnancy loss (SA) and two/three or more losses (RM[≥2] and RM[≥3]). This information may provide effective genetic counseling to the affected couples and help them to decide further reproductive options.
Most of SA or RM are caused by chromosomal abnormalities in the embryo or fetus [16]. As shown in Tables 1 and 3, there was a statistically significant difference in the frequency of abnormal cases in RM group compared with SA group (P=0.046 or P=0.038). The percentage of chromosomal abnormalities was 50.6% in SA and 64.0% for ≥2 pregnancy losses and 65.4% for ≥3 pregnancy losses in RM. This rate of chromosomal abnormalities in RM is higher than that of chromosomal aberrations reported by previous studies, in which reports the incidence of fetal chromosomal aberrations varied between 25% and 57% [8,17,18,19,20]. Stephenson et al. [8]. also reported that women <36 years of age with RM have a higher frequency of euploid miscarriage, which are not consistent with this study. The higher frequency of euploid miscarriages suggests that there are non-cytogenetic factors associated with maternal causes. The maternal causes are well known and include: uterine factors, antiphospholipid syndrome, possibly hereditary thrombophilias, alloimmune factors, infections, and endocrine abnormalities [21]. The fact that patients identified with non-cytogenetic factors were excluded in this study may be one of the explanations about these discrepancies. However, the frequency of euploid miscarriages in both groups of this study was still high and therefore the possibility that there were some cases with non-cytogenetic factors was not completely ruled out.
Although there was a limitation to diagnose the exact gestational age of fetal demise, the present study showed that in SA group, normal (euploidy) miscarriages were increased and miscarriages with chromosomal abnormalities were decreased in proportion to the estimated gestational age (Table 3). The frequency of chromosomal abnormalities is an important issue in RM and seems to depend on the gestational age at time of fetal death. In contrast to the clinical (≥6 weeks) miscarriages, 70% of preclinical (<6 weeks) miscarriages are reported due to a chromosome abnormality [22]. Conversely, the frequency of miscarriages with chromosome abnormalities decreased in second and third trimester pregnancy losses [23].
The most common chromosome abnormality in miscarriages before 10 weeks of gestation is autosomal trisomy, followed by ployploidy such as triploidy or tetraploidy and monosomy X [4], which is consistent with the present study. Trisomies are generally derived from non-disjunction during maternal meiosis, which is strongly associated with maternal age [24].
The abnormal behaviour of centromeres has also been suggested to predispose to meiotic non-disjunction, affecting all chromosomes in couples with RM [25]. Although there should be a corresponding monosomy for each trisomy, monosomy is rarely detected in clinical miscarriage except chromosome X, suggesting that autosomal monosomies are unlikely to be compatible with survival. Polyploidy mainly originates from fertilization by polyspermy or postzygotic division error [26]. In monosomy X, the lack of X chromosome mostly derives from paternal meiotic division error of sex chromosomes [26]. Structural rearrangements and chromosomal mosaicism due to postzygotic errors are occasionally detected in miscarriages. In case of balanced structural rearrangements, one of the parent usually has the same rearrangement and the cytogenetic cause for miscarriage is deniable, whereas de novo occurrence of balanced structural rearrangements might be associated with abnormal phenotype owing to possible gene interruption [27]. All autosomal trisomies except trisomies 13, 18, 21 have been known to miscarry at early stage of gestation. However, an exception in this study was one case of trisomy 9, which was terminated at 18 week gestation.
Little is known on the karyotype of miscarried conceptuses in couples with RM carrying a structural chromosome abnormality, since cytogenetic analysis in these couples is not routine practice. It has been described that after natural conception in carrier couples with RM, approximately 25% of the miscarried conceptuses has an unbalanced karyotype [28,29]. In couples with RM, the incidence of either of the partners being a carrier of a structural chromosome abnormality is 3% to 4%, mainly consisting of reciprocal translocations (61%) and Robertsonian translocations (16%) [30,31]. However, these miscarriages derived from structural chromosome abnormality of parents were excluded in this study.
RM continues to be a challenging reproductive problem for the patient and clinician. Therefore, identifying a cytogenetic cause for a miscarriage may be of great significance for the management of SA or RM patients. In case of detected chromosomal aberration, the patient should be counseled individually according to the type of anomaly. This study should help physicians working in the region to realize the contribution of chromosomal abnormalities to cases of repeated fetal loss. It should also be informative to the patients in understanding why the pregnancy loss occurred, and hopefully assist with associated grief and loss and in decision-making in regard to trying again.





 XML Download
XML Download