

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
During pregnancy and lactation, a woman's breasts face several physiological changes. These changes can be attributed to various hormones, which may also cause vascular hyperplasia and hyperplastic lobules [1]. Such changes may hinder the interpretation of physical and medical imaging examinations of the breasts. It is important to note that most breast lesions that are diagnosed during pregnancy and lactation are benign; however, the different diagnosis of breast cancer is challenging during these periods. Therefore, the aim of this article was to review the changes occurring in the breast, which are related to pregnancy and lactation, and to identify methods for the different diagnosis and treatment of breast disease.
Breast changes during pregnancy and lactation
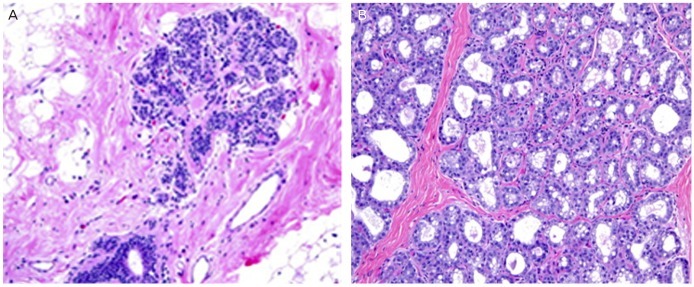
Breast begins to change under the influence of estrogen, progesterone, and prolactin from the mid-term in the first trimester of pregnancy. Particularly, by the influence of estrogen the blood vessels show remarkable growth, and lobules are proliferated. For the meantime, fibrolipoma substrate decreases, blood flow increases, and infiltration of mononuclear cell are often accompanied. During the second and the third period of pregnancy, the proliferation of lobules and the decrease in the substrate become more apparent. Normally, due to progesterone, cell proliferation in the unit of lobule appears apparently, and due to estrogen, the ductal proliferation comes to be much intense. Under the influence of the hormones prolactin and oxytoxin (secreted by the posterior pituitary gland), during late pregnancy, the alveolar cells produce early breast milk called colostrum by taking up nutrients from the blood. Foremilk and hindmilk, whose compositions are different from that of colostrum, are subsequently produced with the help of the hormone progesterone (lactogenesis I). In a period of lactation, due to drastic reduction of progesterone, prolactin levels increase. Shape of myoepithelial cell becomes much thinner and flatter, and along with insulin, thyroid hormone and other metabolic hormones, the myoepithelial cell synthesizes the basic nutrients of breast milk-fat, lactose, and protein (lactogenesis II). During a period of lactation, breast displays the lobular expansion as well as the accumulation of ductal secretion (Fig. 1). The breast milk is secreted by oxytocin and neuroendocrine interactions. To producing of breastfeeding constantly being generated during a period of lactation, a certain amount of oxytocin from the posterior pituitary needs to secrete by stimulating that comes from sucking (lactogenesis III) [2-6].
It takes three months after discontinuation of breast-feeding in order to pre-pregnancy state, and during this process pronounced atrophy of lobules is detected [3].
Imaging and biopsy during pregnancy and lactation
In this period, it is very difficult to distinguish between tumor and normal breast by clinical examination or imaging test. Since the breasts continue to grow and feel firm and nodular during pregnancy, it is possible that a tumor mass may appear as normal tissue during this period. Furthermore, as the breast increases its size, the tumor mass may be located deeper, making it more difficult to identify via palpation.
1. Mammography
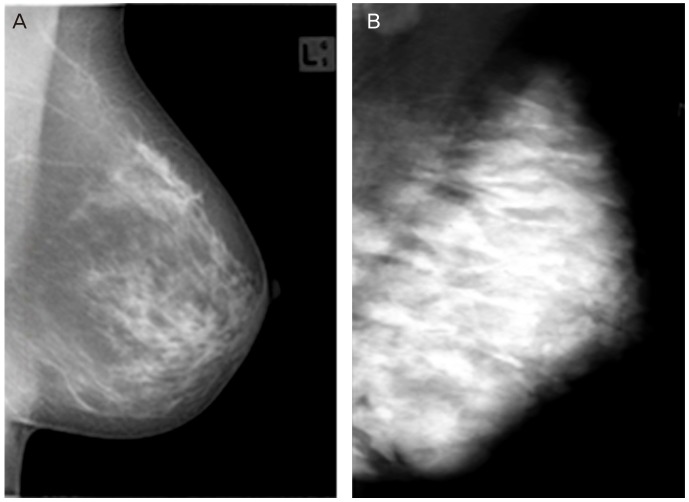
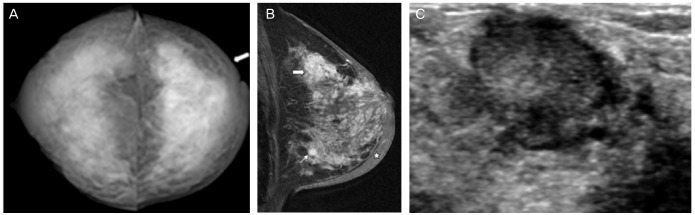
The physiological changes as stated above proliferates the breast parenchyma so that it increases the size, and increases the density of cells, blood vessels, or amount of moisture, therefore, the mammographic parenchymal density increase and diffuse (Fig. 2). Especially, during the lactation period, breast parenchymal density is further increased so that expansion of the lactic duct seems to be nodular and hyperdensity appearance by breast milk filling nipples. Therefore, in pregnant and lactating women, it is difficult to diagnose a tumor by mammography because of the architectural distortion and asymmetric density of the tumor. In such cases, ultrasonography is a more suitable diagnostic procedure than mammography. If a biopsy is indicated by ultrasonography, further mammography must be performed to identify the range of lesions, including microcalcification lesions [7-12]. It is thought that fetal abnormalities, which may occur due to radiation during pregnancy, would appear in case of more than 0.05 Gy. Yet, the radiation that fetus can receive through the mammography introduced in 4 times, is very small as 0.004 Gy, even if one does not wear lead aprons [13-15]. However, except special cases, it is recommended not conduct radiation tests during the first quarter of pregnancy.
2. Breast ultrasonography
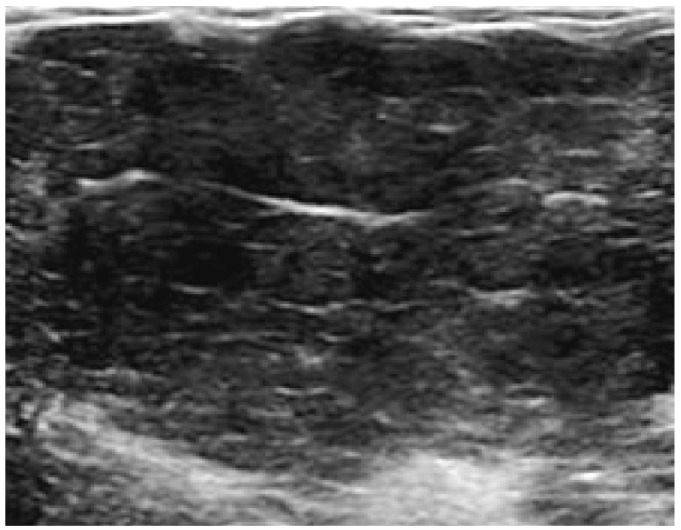
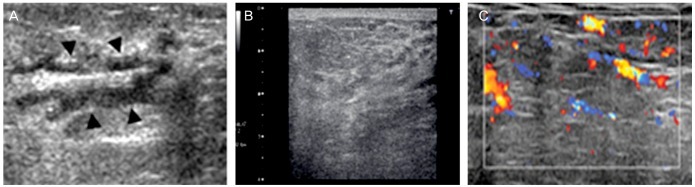
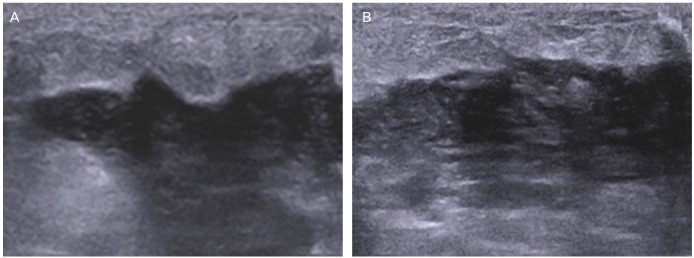
One of the characteristics of breast ultrasonography conducted during pregnancy is that nonfatty fibroglandular tissue with diffuse feature becomes larger, as showing hypoechogenicity (Fig. 3). The other is that during a period of lactation, the nonfatty fibroglandular tissue displays hyperechogenicity, and both vascular tissue and vascular characteristic increase (Fig. 4) [7-11]. Ultrasonic waves can be used as the most dependable medical imaging examination to diagnose pregnancy and breast diseases that may appear during lactation period. In case of malignant breast lumps, ultrasonic represents its higher sensitivity against the lumps, rather than mammography [8,9]. It is known that pregnancy-associated breast cancer (PABC) occupies approximately 3% of all breast cancers. About 90% of PABC show lumps that are possible to be easily diagnosed by ultrasonic.
3. Magnetic resonance imaging
It is not recommended to use magnetic resonance imaging (MRI) as a general inspection for the diagnosis and treatment of breast disease during pregnancy. According to American College of Radiology, in terms of diagnosis of breast diseases during pregnancy, MRI should only be used in cases that it would be regarded to have obvious benefits. It is also said that except special cases, contrast media should not be used [16]. However, in recent studies, it was reported that contrast media would not be closely related to foetal abnormalities [17,18].
European Committee on Radiation Risk reported that gadolinium based contrast could be safely utilized during pregnancy, because it would be less absorbed into placenta and also, it would be rapidly excreted to kidney [19].
4. Cytologic examination
Since the mammary epithelial cells undergo several cellular morphological changes during pregnancy and lactation, a false-positive result may be obtained during the diagnosis of breast cancer. Therefore, the results of these diagnostic procedures must be carefully interpreted. A core biopsy examination of the suspected malignant lesion must be conducted and interpreted by a skilled pathologist [20,21].
5. Core biopsy
Core biopsy, most appropriate method of tissue diagnosis in pregnancy and lactation period, is safe and economical (cost-effective). The process of breast milk production is characterized by increased blood flow to the breast, which increases the risk of bleeding, and expansion of the milk ducts increases the risk of infection, which can cause a milk fistula because breast milk is generated in this stage. Milk fistula is known to occur more in central than in peripheral. Thus feeding temporarily suspend before aseptic surgery and a biopsy, biopsy is in the correct location and after the procedure, hemostasis using compresses or ice packs will help [22].
Breast disease related to pregnancy, lactation period
1. Benign breast disease associated with physiological change
1) Gestational and secretory hyperplasia
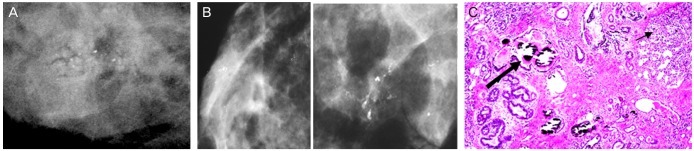
Microcalcification can be the result due to gestational hyperplasia associated with pregnancy and secretory hyperplasia associated with breast-feeding in mammography. This calcification looks mostly round and focal or diffuse distribution, but rarely shows a irregular, linear distribution, branching pattern. Round and small punctate calcifications represent lobular acinar proliferation and linear distribution represents the growth of the cannulated (Fig. 5) [23-25].
2) Spontaneous bloody nipple discharge
Bloody nipple discharge does not occur commonly in pregnancy or in a period of lactation. However, it can be cause by even small stimuli because the blood flow in breast increases rapidly and the change of epithelial cells gets even worst in 3rd trimester of pregnancy. Slight bloody nipple discharge can be seen from approximately 20% of nipple discharge during pregnancy and 15% of a period of lactation [26]. This phenomenon mostly stops as the lactate feeding begins, but also has a possibility of a severe case that may persist throughout the whole lactation period. Diagnostic cytology tests must be performed for the wounds of nipples by feeding. If the result, physical examination and ultrasound are normal, the follow up test should be recommended in a timely manner.
3) Galactocele
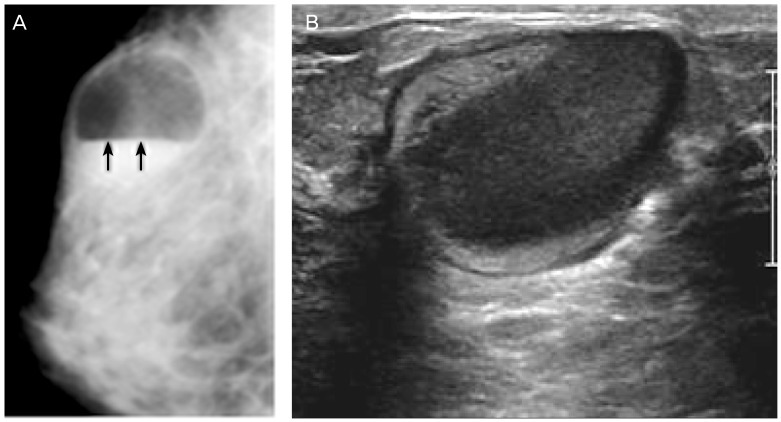
Galactocele is a benign lesion, which is mostly detected after a few weeks or months from the time the patient stopped breast feeding, or during lactation or during the 3rd trimester of pregnancy [11,29]. This means it is surrounded by the epithelial cells and myoepithelial cells and contains liquid that is similar to lactate in cystic changed terminal duct and ductules. Most of the galactoceles are found as painless palpable mass which contains protein, fat, lactose in aspiration analysis and are often accompanied by inflammation and necrosis. Therefore, it is considered that the galactocele is formed by the wall fibrosis due to the inflammatory response of extension of lactate ducts. When the contents leak within the breast, chronic inflammation and fat necrosis are observed [30]. Needle aspiration biopsy is helpful for diagnosis and treatment, however, milk-like liquid during lactation and sticky milky contents after lactation, are found in aspiration [29,31]. If it recurrs even after several aspirations, imaging test is needed. Depending on the proportion of fat and protein in breast milk, mammographic findings of galactoceles may vary, which can be seen as follows.
(1) Pseudolipoma: When a higher fat content, seems to be completely radiolucent mass.
(2) Cystic mass with fat-fluid level: Low concentration of fat content rises up and the liquid sinks to the bottom. It is a diagnostic finding that is seen in the mediolateral oblique view of Mammography.
(3) Pseudohamartoma: Galactoceles does not separate lipid from liquid and it is seen radiologic findings which is simliar to hamartoma that contains high viscosity of breast milk [31].
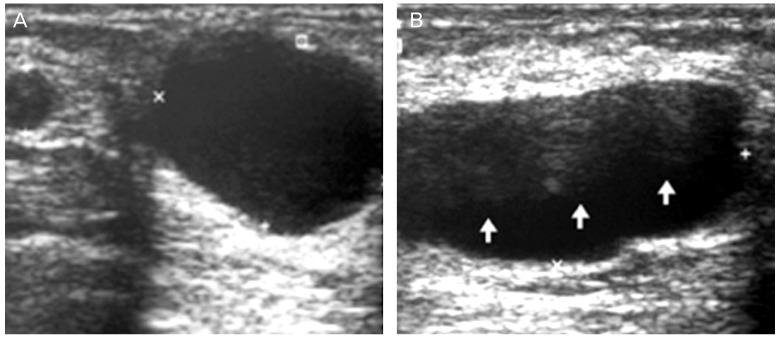
Sonographic findings of galactoceles may also vary depending on the time and site of lesion. In the acute phase, it may appear as an anechoic unilocular simple cyst or a multilocular cyst with thin septation. It is common multilocular cyst that occurs in peripheral region and it is common unilocular or bilocular cyst that occurs in central region. The intensity of hypoechoic echo increases gradually due to the interface between the fat and water components. In this case, Doppler examination performed by the blood vessels in the center to make sure that no particles moving when you press the transducer lesions may be helpful in the diagnosis. In ultrasound, galactoceles only breast milk composition consists of benign solid masses as shown boundaries if and posterior acoustic enhancement seems clear. A long time later, several ingredients are mixed and if you look inside looks mixed echogenic heterogeneous mass (Figs. 8-10) [11,32-34]. Galactoceles is rich in nutrients, and sometimes it can be infected. This finding is well observed in the ultrasound. Aspiration here, you can see that the purulent fluid and breast milk ingredients are mixed in (Fig. 11). Most natural decay takes over several weeks, but occasionally a more long-lasting.
2. Inflammatory and infectious diseases
1) Postpartum mastitis (puerperal mastitis)
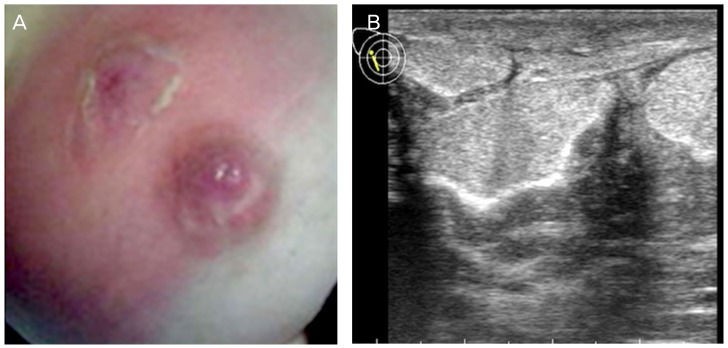
It's not common to see infections during pregnancy, but it is often observed in lactation. Staphylococcus aureus and Streptococcus, which are common pathogens present in the nose and throat of newborn babies, may infect the breast via the damaged epithelial cells of the nipple-areola complex during breast feeding. Nipple cracks or abrasions of the skin can be often discovered on the patient's past history. If breast milk is stagnant, it would be a good culture medium and cause symptoms [24,29,30]. S. aureus infections, being topical, result in severe clinical symptoms right from the beginning, whereas infections caused by streptococci are diffuse and cause local abscess only in the advanced stage of infection (Figs. 12,13). It is treated well by antibiotics, especially amoxicillin-clavulanate. It is quite rare, but puerperal mastitis by methicillin-resistant S. aureus can be very fatal [35-37]. Mammography should not be performed, unless there are suspicious malignant findings. The reason is that it mostly shows thickening of the skin and fibrous tissue even though it is very severe mastitis. Moreover, it is rare to discover other severe abnormalities. If there is abscess formation suspected, the ultrasound examination is first required for the diagnosis and treatment. Irregular boudaries, hypoechoic or anechoic mass, thick, irregular walls, posterior acoustic enhancement, and liquid debris (fluid-debris) shades can be observed in the abscess. Sometimes the air in abscess can cause bright reflection. These hyperechoic dots floating point is the differentiation of malignant. Mastitis in lactation abscess developed in the subacute form, periarthritis [38,39]. Abscess is easily treated by incision drainage. If the abscess lesion size is less than 3 cm, it can be treated with 14 to 21 gauge needle aspiration. If the abscess lesion size is 3 cm or more, it can be aspirated with the 6 to 8 Fr catheter drainage or surgical drainage. Before doing this, it is important to dry up the abscess first. It is necessary that examiner should irrigate the cavity with normal saline under local anesthesia after the drainage to prevent recurrence [38-40]. After treatment, continuing breast feeding helps improve inflammation and promote drainage. Also, breast feeding can be safely performed during antibiotics therapy [29,35]. If there is no improvement despite these treatments, examiner should suspect tumor and perform cytology test and biopsy.
2) Granulomatous mastitis
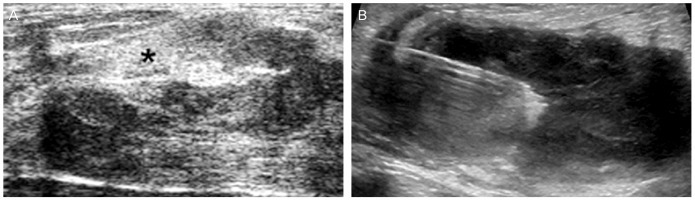
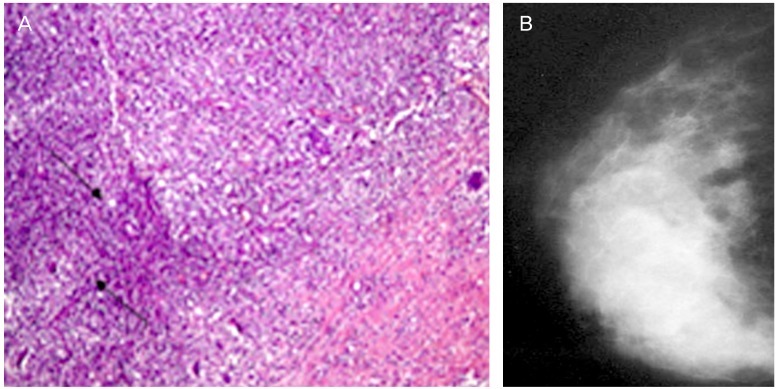
Granulomatous mastitis occurs mainly in young women, and it is an uncommon type which mainly occurs within five years after pregnancy [41-43]. It exhibits specific histological findings characterized by non-caseating (noncaseating), non-vascular (nonvasculitic) granulomatous inflammatory changes, which can be noted in the center of the lobules. Mammographic findings are diverse from normal to benign with focally asymmetric shadow and malignant. Sonographic findings helpful in diagnosis are multiple appearances, which often show hypoechoic and sometimes large hypoechoic mass in adjacent lactiferous gland (Fig. 14) [43]. However, it requires special attention in diagnosis because it is not well differentiated from malignancy, and reactive lymphadenopathy is observed in about 15%. Local excision can be a treatment [40-46], but sometimes it disappears naturally. Therefore close follow-up is necessary [47].
3) Juvenile papillomatosis of the breast
Benign proliferative lesion is a common type because of the influence of hormones during pregnancy and lactation. Juvenile papillomatosis of the breast rarely occurs in young women, and it is characterized by ductal hyperplasia and papillary proliferation of the wall surrounding its sac [48]. It is seen as a hypoechoic mass with an unclear margin in an ultrasonogram, and no specific findings, except an asymmetric shadow, is seen in a mammogram; however, sometimes microcalcification can be observed. The treatment is a surgical resection. It is important to check if the resection margin is completely negative when it comes to preventing recurrence.
3. Benign tumor
1) Tumors related to pregnancy and lactation
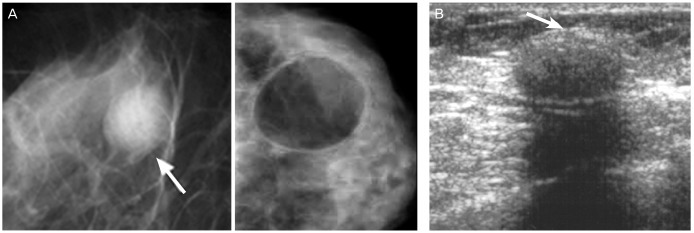
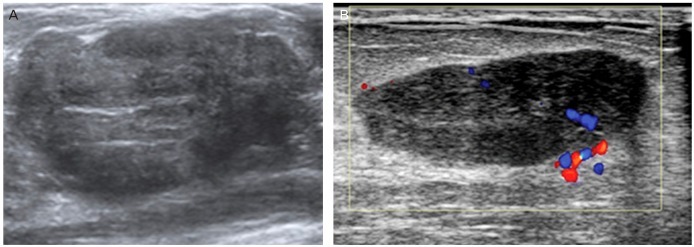
Lactating adenoma is a benign tumor mainly caused by the physiological changes that occur during pregnancy and lactation. This typically occurs during feeding or the third trimester of pregnancy. Lactating adenoma is sometimes interpreted as a variant of fibroadenoma, tubular adenoma, or lobular hyperplasia, which are also caused by physiological changes [49-51]. Fibroadenoma is mixed with stromal and epithelial components. Lactating adenomas, however, only consists of epithelial component. Grossly, it seems to be a certain boundary and elastic mass. Histologically, it is densely packed with lobules, which are separated from each other by a thin connective tissue. Lactating adenoma is composed of acinars and mature thin tubes and filled with secretion is softer than a fibroadenoma The physiological changes that occurs in the surrounding normal parenchyma takes place in the lesions of the internal secretion and secretory hyperplasia appears [49-51]. Lactating adenoma can naturally disappear at the end of pregnancy or lactation. It may also disappear by necrosis, like a fibroadenoma [52]. Most of Lactating adenoma does not relapse after complete resection. Lactating adenoma accompanying malignant lesions is very rare. And it does not increase the risk of breast cancer. It is difficult to distinguish between a lactating adenoma and a fibroadenoma by imaging. A radiolucent or hyperechoic area, which indicates fat content of breast milk, according to lactation hyperplasia, can be seen on mammography or ultrasonography and is useful in diagnosis (Fig. 15). It appears to be a small hypoechoic mass, which is difficult to distinguish from the surrounding tissue on ultrasonography. Moreover, because of its posterior acoustic enhancement and hormonal changes, it appears hypervascular in color or output Doppler. Occasionally, the differential diagnosis of malignant lesions is difficult mainly due to unclear boundaries, microlobulated periphery, reducing posterior acoustic effect, structural heterogeneity. And it occurred by the necrosis of lactating adenoma [11,53-55].
2) Morphologic and physiologic changes in fibroadenomas secondary to pregnancy and lactation
(1) Growing fibroadenoma
Fibroadenoma is the most frequent lesion found during pregnancy and the period of lactation. It can be formed before pregnancy, however, there are many instances wherein it is undetected because it is not palpable or breast screening inspection is not performed on young women. Fibroadenoma increases in size during pregnancy because of its sensitivity to hormone levels. Imaging findings of fibroadenoma is not very different during pregnancy, however, findings such as dilation of lactiferous ducts and increase in blood of flow is very similar to complex fibroadenoma (Fig. 16) [29,56,57]. When performing fine needle aspiration for diagnosing palpable fibroadenoma, you must consider the physiological changes of cells during pregnancy [58]. Central biopsy is also appropriate and must be carefully done to avoid hemorrhage, lacto fistula and infection.
(2) Fibroadenoma with infarction
Spontaneous necrosis of fibroadenoma is very rare, but it is sometimes observed during pregnancy or lactation. It can be presumed when there is sudden pain during the third trimester or during birth. The cause is embolism within the vessels and it shows more borderlines of lobules and mixes echos and shows posterior shadow depending on the degree of necrosis. If necrosis is more extensive, central biopsy must be performed to differentiate from a malignant lesion [30,59-61].
(3) Fibroadenoma with secretory hyperplasia or lactational change
During pregnancy, hormone-sensitive breast parenchyma of fibroadenoma is stimulated by pregnancy hormones leading to secretory hyperplasia. This is very similar to the phenomena seen in lactating adenoma, so it is very difficult to distinguish between both. When fibroadenoma undergoes changes during lactiferous phase, there can be lactation during sucking and it is noted that this phenomena is not seclusive to breast cysts. Similar to complex fibroadenoma, it is diagnosed based on the findings of secretory hyperplasia, which appears as mixed echo, and dilated lactiferous ducts and cysts. Furthermore, calcification may sometimes be detected during breast imaging.
4. Malignant tumor (PABC)
1) Introduction
PABC is defined as breast cancer that occurred during pregnancy and after delivery within one year, represents up to approximately 3% of all breast cancers, occurring in one incidence per 3,000 to 10,000 pregnancy. Delay of childbirth age shows increased prevalence and advanced stage at the time of diagnosis and poor prognosis and seems that more than 50% are high-grade tumors [29,62,63]. And large number of them are form of inflammatory tumor and shows in more than 50% lymph node metastasis, negative at hormone receptor and positive at HER2/neu [62,63]. Late diagnosis of tumors owing to the biological effects of pregnancy results in poor prognosis and rapid tumor growth; recurrence is common within 2 to 3 years of the diagnosis [29,62,63].
Mostly palpable lesions and clinical symptoms are visible swelling, redness, and diffuse mastosis at locally advanced carcinoma [29,62,63]. The imaging findings of breast cancer in non-pregnant women are not significantly different from those in pregnant women due to the increase in glandular density. Even in non-pregnant women, mammography has low sensitivity, and ultrasound is considered a better diagnostic tool [7-12].
2) Cause of delayed diagnosis
The mammary gland undergoes clinical and physiological changes during pregnancy, making imaging diagnosis difficult. The majority of patients with advanced stage looks so delayed diagnosis is as follows [64,65].
Young women who are not a screening test.
Self-examination is difficult and is not performed frequently.
The clinical examination is difficult because of increased blood flow and dense mammary tissues.
Until delivery they are not good at follow up test.
Breast care at the department of obstetrics and gynecology does not enforce.
Reluctant to biopsy during pregnancy.
During pregnancy is known to be delayed an average of 5 to 7 months of breast cancer diagnosis, whenever be delayed one month diagnosis shows increased by approximately 0.9% to 1.8% of axillary lymph node metastasis [66].
3) Symptoms
In most cases, it appears as a breast mass with no associated pain, and sometimes, it can be found on breast examination in the absence of breast feeding [66]. During the third trimester of pregnancy, hemoid secretion is often seen due to loss of epithelial cells alike papilloma in lactiferous drifts and this is a common symptom.
Cytological examination will be carried out when hemoid secretion is continued more than 2 months after delivering.
4) Diagnosis
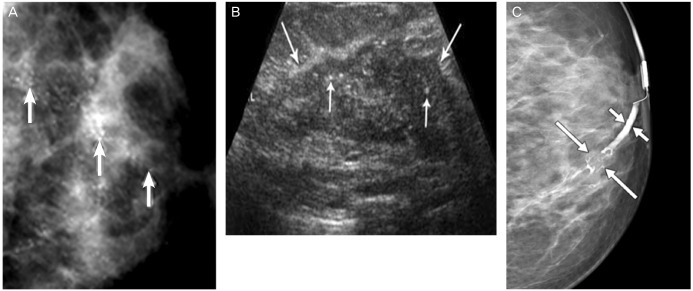
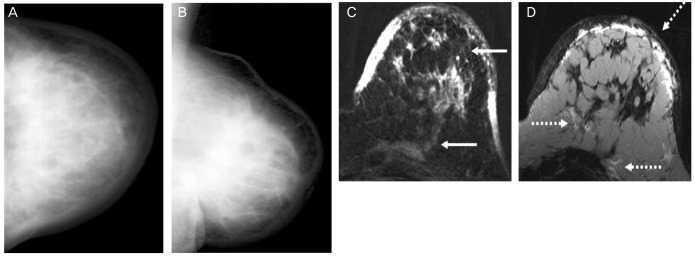
Although mammography is not effective in pregnancy because physiological changes decreased sensitivity and specificity, it is performed suspected malignancy. 68% to 74% of PABC has abnormal findings with mammography and 90% of PABC has Breast Imaging Reporting and Data System (BIRADS) 3 to 4 score. During pregnancy, ultrasound seems the most effective imaging studies in the diagnosis of breast disease. And it's sensitivity to the breast disease is 93% to 98% (Figs. 17, 18). Complex echo pattern, posterior acoustic enhancement is a common finding in the PABC compared with non-pregnancy breast cancer. Necrosis or cystic change is seen in the carcinoma present non-echo pattern and posterior acoustic enhancement because tumor grows up quickly by stimulation of the hormonal changes in pregnancy.
5) PABC in carrier with BRCA mutation
Carriers with breast cancer (BRCA)1 or BRCA2 mutation are at high risk for breast cancer. Therefore carriers with BRCA1 or BRCA2 mutation certainly needs to undergo strict clinical and image examination before and after pregnancy. This strict examination uses ultrasonography and MRI, but ultrasonography is more useful than MRI because the latter is difficult to find during the period of lactation (Fig. 19).
According to former studies, the PABC prevalence of carrier with BRCA1 mutation is higher than BRCA2 mutation [67]. Carriers of mutations in the BRCA1 or BRCA2 genes who have parity have an increased risk of PABC than those who do not have parity before the age of 40 years, and pregnancy at an early age does not decrease the prevalence [68]. But it was recently reported by International BRCA1/2 Carrier Cohort Study (IBCCS) that carriers with BRCA1, BRCA2 malignant and control group has decreased the risk of being malignant after the age of 40 years [69].
6) Treatment
(1) Pregnancy interruption
In the past, due to the adverse affects of tumor growth and proliferation due to increasing hormone levels during pregnancy, therapeutic abortion was encouraged. But according to several studies, the therapeutic abortion does not improve the prognosis. The reason is that the mammary gland of most of PABC is hormone receptor negative and imcomplete growth and division occur in the point at which the pregnancy ends. For this reason therapeutic abortion brings about growth of tumor. So termination of pregnancy should be considered in case of a very aggressive tumor or receptor positive.
(2) Staging and histologic types
According to stage by Tumor-Node-Metastasis (TNM) system of American Joint Committee on Cancer, the most common histologic type is infiltrating ductal adenocarcinoma for 80%.
(3) Surgical treatment
During pregnancy axillary disection can be performed safely with modified radical mastectomy and lympectomy. Breast parenchyma can be preserved in the following 2 ways during pregnancy. First, conserving surgery can be performed in the second trimester of pregnancy, and radiation therapy, after delivery. Second, conservation therapy and neoadjuvant chemotherapy can be performed in the second trimester, and radiation therapy, after delivery.
(4) Chemotheraphy
The majority of anticancer drugs that are administered to a PABC patient can cause teratogenesis and mutation that are related to intrauterine growth retardation (IUGR), deformity, still birth. Teratogenesis increases 20% especially in the first trimester of pregnancy. Furthermore, due to the physiological changes during pregnancy, i.e., increased renal blood flow, glomerular transmittance, and creatinine, the pharmacokinetics of a cytotoxic drug are altered. Moreover, the drug may be accumulated in the amniotic fluid, which may interrupt its excretion. In general, the cytotoxic drug crosses the placenta, but do not know how to pass suspension. However, because teratogenic in first trimester, 5 to 10 weeks attention and 13 weeks after the safety. Methotrexate is prohibited because of the high risk of contraindication for teratogenesis and miscarriage. Drugs belonging to Food and Drug Administration category D, such as cyclophosphamide, fluorouracil, and cisplatinum, affect teratogenesis in the first trimester, but rarely have an adverse effect during the second and third trimesters. In general, taxanes and trastuzumab are considered safe during pregnancy; however, more studies are needed to confirm their safety.
(5) Hormone therapy
Most PABC are hormone receptor negative, and in these patients, it is necessary to administer tamoxifen. However, this medicine is prohibited during pregnancy, because it is related to colporrhagia, natural abortion, stillbirth, and malformation. If necessary, it would be recommended to use after the delivery [70].
(6) Radiotherapy
Even a little radiation, which can be hardly detected, could be fatal to the infant. Pregnant women are most sensitive to radiation during the first 10 to 38 days of pregnancy. During this period, radiation can cause fetal abnormalities such as microencephaly, anencephaly, ocular damage, and clubfoot.
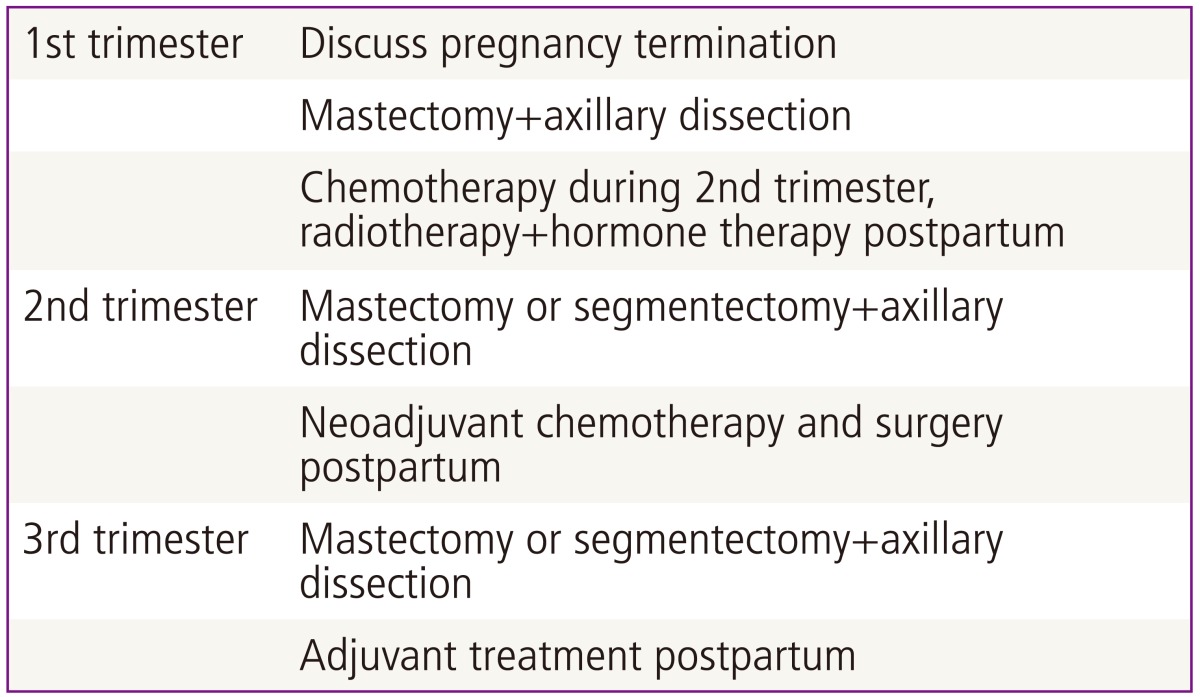
According to the pregnancy period, Mother's body surface is increasing. Therefore, the quantity of the radiation which the infant absorbs depends on the physiological changes from Mother. For example, if radiation of 5,000 cGy is measured in Mother's breast, the infant is exposed to the radiation of 10 to 15 cGy in the first-quarter and to the radiation of more than a hundred in the third-quarter. Consequently, it is recommended that radiotherapy should folllow after giving birth (Table 1).
Conclusion
Breast lesions that are detected during pregnancy or nursing are not very different from those detected in non-pregnant women. But, it is difficult to diagnose these lesions in pregnant women due to the hormone-induced physiological changes occurring in the breast.
However given enough understanding and knowledge about special clinical and imaging features in pregnancy and having aggressive approach or action toward these symptoms accordingly it will be helpful to treat and diagnose.


 XML Download
XML Download