

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Uterine cervical cancer is the second most common malignant tumor, accounting for about 15% of all female cancer worldwide. Annually 400,000 patients are newly diagnosed, and 250,000 die from this disease globally. Although the overall incidence of the disease is decreasing, 3,616 new cases were diagnosed in 2007 in Korea, and the incidence of cervical cancer is still higher in Korea than in other developed countries according to the research data of the National Cancer Information Center from May 2010 [1].
Although Papanicolaou (Pap) smear has significantly contributed to the decreasing incidence and mortality of cervical cancer [2], a large number of women still suffer from this disease in both developing and developed countries. Furthermore, uterine cervical cancer is also found in women who have received regular periodic testing [3]. It is thought that the low sensitivity of the PAP smear test causes errors in cervical sampling and the interpretation of atypical cells [4]. Therefore, it is clear that development of a more accurate biologic marker is badly needed to improve the sensitivity and specificity of the screening test process in diagnosing uterine cervical cancer.
Cervical cancer develops by multilevel cancer steps. It is well known that the high risk human papilloma virus (HPV) is closely related to the onset of cervical cancer. Persistent HPV infection can cause cervical dysplasia and contribute to cancer development by affecting the restoration & apoptosis of damaged cells. That is, HPV E6 destroys p53 [5] and HPV E7 inactivates products of rentinoblastoma (pRB), and this can increase the expression of p16INK4A [6]. p16INK4A is involved in the G1 cell cycle which is an important stage for the repair and extinction of damaged cells. Accordingly, it is suggested that expression of p16INK4A can help in screening tumor cells.
Galectin-3 is one of the genetic families widely distributed in carbohydrate binding hormones, expressed variably in tumor cells and involved in cellular growth, differentiation, inflammation, apoptosis and metastasis [7-12]. It has not yet been shown definitively how galectin-3 affects tumor progression but it is clear that expression of galectin-3 differs according to the type of tissue from which a tumor arises [13,14]. The author compared the expression of p16INK4A and galectin-3 in normal uterine cervix, precancerous lesions including low grade squamous intraepithelial lesions (LSILs), high grade squamous intraepithelial lesions (HSILs) and invasive cancer to determine if there is some difference between these lesions.
Materials and Methods
1. Tissue samples
We obtained tissue samples from patients who underwent uterine cervical biopsy or hysterectomy in Kangnam Sacred Heart Hospital between 2005 and 2009. The tissue was prepared with formalin and embedded in paraffin, and then an H&E stain was done. All tissue was thoroughly examined by pathologists. We selected 20 cases of normal tissue, 17 cases of LSIL, 26 cases of HSIL, and 24 cases of invasive cancer at random.
We selected squamous cell lesions rather than other cell lesions because squamous cell lesions are the most common pathologic type in the cervix. Normal cervical tissue was obtained from 20 patients who had undergone hysterectomy due to conditions other than cervical lesions.
2. Immunohistochemical staining of p16INK4A & galectin-3
We obtained sections 4 µm thick from paraffin-embedded tissue samples. These sections were attached to slides and deparaffinated with xylen, and then hydrated by degrees with 100%, 90%, and 75% alcohol.
The slides were inserted in 0.1 M citric acid solution (pH 6.0) and microwaved 4 times for 20 minutes. All slides were then treated with 3% hydrogen peroxide for 15 minutes, to inactivate the hydroperoxide enzyme. Then, galectin-3 and p16INK4A were treated with a protein blocking solution for 10 minutes and 20 minutes each and washed with a pH 7.6 Tris buffer solution.
A primary antibody was applied to p16INK4A (monoclonal, Neomarker, Fremont, CA, USA; 1:100) and galectin-3 (Abcam, Cambrige, UK; 1:50) for 1 hour then washed 3 times with a Tris buffer solution.
HRP EMV kit (Dako Co., Glostrup, Denmark) was applied for 30 minutes at normal temperature, washed 3 times with Tris buffer solution. Then, ager was done by applying 3, 3-diaminobenzene for 5 minutes. The stained slides were cleaned with distilled water and the contrast stain was done by hematoxylin, before the mounting was done.
3. Interpretation of staining results
We examined all the slides with an optical microscope at ×100 field and also examined the checked number of cells, which presented positive at ×400 field. Two independent observers evaluated the staining of the slides and we analyzed the proportion and intensity of the staining responses in the cell and nucleus. In p16INK4A, a proportion of stained cells < 1% means 0, 1-4% means 1 +, 5-25% means 2 +, 25-75% means 3 +, and > 75% means 4 +. In galectin-3, proportion of stained cells < 5% means 0, 5-25% means 1 +, 25-50% means 2 +, 51-75% means 3 +, and > 75% means 4.
4. Statistical analysis
A one-way analysis of variance (ANOVA) was used to evaluate the differences in the expression of p16INK4A and galectin-3 between normal and abnormal tissue, including LSIL, HSIL, and invasive cervical cancer. Analysis was done by SPSS 15.0. P-value < 0.05 was statistically significant.
Results
1. Expression of p16INK4A protein
The proportion of p16INK4A expression was negative in 95% cases of normal epithelium, and the mean value was 0.1. In LSILs, the proportion was 1 + or 2 + in 76.5% and the mean value was 1.35. There was no negative response, 1+ or 2+ in HSILs. 3 + comprised 57.7% and 4 + was 42.3% of cases of HSILs, and the average value was 3.42. In invasive cancer, = 3 + was 100%, 3 + was 20.8%, 4 + was 79.2%, and the average value was 3.79 (Fig. 1). There was a statistical significance between the proportion of p16INK4A protein expression and the grade of uterine cervical lesion (P < 0.05) (Table 1).
2. Expression of galectin-3 protein
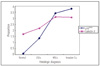
The proportion of galectin-3 expression was negative, 1 +, or 2 + in 95% cases of normal epithelium, and the average value was 1.70. In LSILs, it was 2 + or 3 + in 94.1% of cases, and the average value was 2.17. It was ≥ 3 + in 80.8% of HSILs, and the average value was 3.11. Although the proportion of galectin-3 was ≥ 3 + in 75% of invasive cancers, the average value was 3.08 (Fig. 2). Therefore no major difference between HSILs and invasive cancers existed in regard to the proportion of galectin-3 expression (P=1.00) (Table 2). However there was a statistical significance between the proportion of galectin-3 expression and the grade of cervical lesions like p16INK4A (P<0.05) (Table 2, Fig. 3).
DISCUSSION
Cervical cancer arises from carcinoma in situ, which originates from precancerous lesions in normal cervical epithelium, or cervical dysplasia.
HPV infection is recognized as the most prevalent cause of cervical cancer. HPV E6 destroys p53 [5] and HPV E7 inactivates pRB, potentially increasing the expression of p16INK4A with persistent HPV infection [6].
p16INK4A gene, a cyclin-dependent kinase (cdk) suppressor factor, regulates the activity of cdk4 and cdk6, and is inactivated by genetic defect or hypermethylation in many types of cancers [15,16]. The role of p16INK4A as a tumor suppressor gene has been reported in many types of malignant tumors such as malignant melanoma, gastrointestinal cancers, and lung cancers. Expression of p16INK4A related to HPV has a different mechanism of expression from other types of malignant tumors. The E7 tumor protein in high-risk types of HPV combines with and inactivates the pRb, tumor suppressor protein, and releases a transcription factor resembling E2F. This transcription factor activates the cell cycle by advancing G1/S phase [17]. p16INK4A expression which is controlled by a negative feedback mechanism, is relatively increased by the inactivation of pRb [18]. There are many reports that p16INK4A is over-expressed in cervical cancer and precancerous lesions infected with high risk types of HPV [18-20]. Since the relationship between HPV infection and p16INK4A expression in immunohistochemical results was first reported by Sano et al. [15] the role of p16INK4A has been widely studied [21,22]. Klases et al. [19] noted the expression of p16INK4A in cervical tissue samples using immunohistochemical staining. They also found that all cervical intraepithelial neoplasia (CIN) lesions other than low risk types of HPV infected CIN, and almost all invasive cervical cancers had a strong expression of p16INK4A. However there was no expression of p16INK4A in normal cervical epithelial cells, inflammatory lesions and low risk types of HPV infected CIN. Furthermore, they also found that there was same expression of p16INK4A in PAP smear of cervical dysplasia. Therefore p16INK4A expression has been considered as a definite biomarker, which can confirm tumor cells in cervical tissue samples and PAP smears. Similarly, in our study, p16INK4A protein was not expressed in 95% of normal epithelium, LSILs had < 25% expression in 94.1%, and HSILs and invasive cancers had ≥ 25% expression in 100%. More than 75% of expression was of higher frequency in invasive cancer than HSIL (78.2% vs. 42.3%). In our results, p16INK4A protein was mainly expressed in HSILs and invasive cancers, therefore immunohistochemial staining of p16INK4A would be helpful in diagnosing cervical lesions.
However Wong et al. [23] have insisted that the p16INK4A expression rate is the result of p16INK4A over-expression by HPV infection. Therefore, further analysis is needed to make clear the relevance of HPV infection to p16INK4A expression.
Galectin-3, 31-kDa, a kind of carbohydrate binding protein, has a chemical affinity to β-galactosides, and has the homology of genetic arrangement in carbohydrate binding lesion [7].
Galectin-3 had been known as Carbohydrate binding protein-35 (CBP-35), Mac-2, L-29, L-34, or L-31. It consists of aminoterminal including repetitive genetic arrangement, which is abundant in leucine, tyrosine & proline, and globular structure including carbohydrate binding lesion [7-14]. Galectin-3 responds to special kind of ligands, and is present in a number of biological steps such as cellular growth, differentiation, inflammation, modification, metastasis and adhesion. Galectin-3 is secreted by tumor cells and macrophages, induces chemotaxis by affecting vascular intraepithelium, and accelerates motility in early stage of tumor formation [11].
The importance of galectin-3 expression in many types of human tumors has been studied. Galectin-3 expression has been found to be higher in pancreatic, gastric, thyroid, head & neck, renal, colon, rectal, liver cancer and leiomyosarcoma than in normal cells. On the other hand, there are conflicting results in regard to other types of tumors. Galectin-3 expression, for example, is lower in breast, ovarian and endometrial cancer than normal cells. In metastatic cancer, the frequency of galectin-3 expression is higher than in primary cancer [24].
The only report regarding the relationship between grades of cervical lesions and galectin-3 expression is by Lee et al. [25] which concluded that galectin-3 expression decreases as the cervical lesion progresses [25].
But our conclusion is contrary to Lee's findings. In our study, more than 50% expression was only found at 5% in normal epithelium, 23.5% in LSILs, and 70-80% in HSILs & invasive cancers.
Additionally, the intensity of galectin-3 expression increased as the cervical lesion progressed to invasive cancer. Thus, we could use galectin-3 immunohistochemical staining as a tool in diagnosing and supposing uterine cervical lesions. But it is thought that larger scale research is needed, in order to consider the rise and fall in galectin-3 expression as cervical lesions progress.
The author used immunohistochemical stains of p16INK4A and galectin-3. p16INK4A is a gene associated with controlling the cell cycle in canceration. Galectin-3 is a kind of carbohydrate binding protein, that is diversely expressed in tumors, and affects cellular growth, differentiation, inflammation, apoptosis, and metastasis. Expression of p16INK4A & galectin-3 increases as the cervical lesion progresses to invasive cancers. This suggests that the expression of p16INK4A and galectin-3 using immunohistochemical stains is associated with the progression of cervical lesions. Therefore, immunohistochemical staining of p16INK4A & galectin-3 would be valuable when used with PAP smear in diagnosing cervical lesions and predicting disease progression. But further research including research focusing on the association between these biomarkers and biopsy results (mild, moderate, severe dysplasia) is needed in the future.




 XML Download
XML Download